Reducing the need for adjunctive antibiotics during scaling and root planing

There has been much attention in the literature and news regarding the overuse of antibiotics in medicine and dentistry. For example, it has been reported recently that antibiotics were given to 30% of older patients with Medicare benefits during outpatient visits for COVID-19 from April 2020 to April 2021, even though antibiotics are ineffective treatments for viral syndromes including the virus that causes COVID-19.1
Periodontal disease is widespread and affects 40% of the US population. Because periodontitis is caused by oral bacteria in the plaque around teeth, dentists often use systemic antibiotics in conjunction with scaling and root planing (SRP) of the teeth (deep cleaning) to achieve disease resolution. Although the research does show some benefit in select patient cases of adjunctive use of systemic antibiotics during SRP, it remains unclear as to who the best candidates are for receiving these antibiotics and the risk-benefit ratio of overprescription.3
Concerns have arisen over indiscriminate use of antibiotics, resulting in strains of resistant bacteria or superbugs. In addition, antibiotics can be associated with considerable morbidity such as drug-induced lupus, Clostridioides difficile colitis, and/or fatal reactions such as anaphylaxis or Stevens-Johnson syndrome.4 Finally, Alzheimer’s disease and Parkinson’s disease are neurogenerative diseases that have recently been hypothesized to be associated with a dysbiosis of microbes in the intestine. It is thought that because antibiotics disturb the balance of intestinal flora, they can be a triggering factor for neurological disorders, including Alzheimer’s and Parkinson’s, especially during old age when immune defenses are lacking or reduced.5
Also by the author:
- Dental implant failure and penicillin allergy, explained
- Pinhole Surgical Technique: A 10-year evaluation of root coverage
Antimicrobial stewardship programs have been discussed that establish prudent administration of antibiotics guidelines across different societies in the medical and dental fields, with the aim of reducing nonevidence-based overprescription.6 In these programs, any protocol or alternative modality that can result in de-escalation of unnecessary antibiotic use is advocated.
The purpose of this article is to describe a pilot study involving 10 patients with moderate to severe chronic periodontal disease slated for four quadrants of SRP that utilized the StellaLife Vega Oral Care Recovery Kit for 10 days prior to initiation of periodontal therapy. The concentration of oral bacterial pathogens was measured prior to use of the recovery kit and then 10 days after use. An overall mean average reduction of 22% in oral pathogen bioburden was recorded, suggesting that the use of the oral care recovery kit prior to periodontal therapy may decrease the need for adjunctive systemic oral antibiotics during SRP treatment.
Rationale for study
StellaLife Vega Oral Recovery Kit consists of a natural oral rinse, oral spray, and topical gel containing herbal extracts of Azadirachta indica, echinacea, calendula, and propolis. The active ingredients in this treatment have been shown to have similar antimicrobial properties to 0.12% chlorhexidine without the cytotoxicity to human gingival fibroblasts and osteoblasts.7 This treatment has also been suggested to enhance oral wound healing by upregulation of collagen type I transcription.8
Another recent in vitro study suggested that StellaLife Vega oral rinse, when compared to 0.12% chlorhexidine, showed bacteriostatic properties without the cytotoxicity and inhibition of human gingival fibroblast proliferation that was seen with chlorhexidine use.9 Other notable side effects with 0.12% chlorhexidine use during periodontal treatment include dysgeusia, staining, increase in tartar accumulations, mucositis, and dermatitis.10 Based on its bacteriostatic properties and its ability to enhance wound healing without the side effects seen with other medicated mouth rinses, a pilot study was created to evaluate the ability of these compounds to reduce oral pathogen bioburden prior to SRP to reduce the possible need for adjunctive systemic antibiotics.
Study
Ten patients diagnosed with generalized chronic moderate to severe periodontal disease (stage III or IV grade B)11 with a bleeding and plaque index of 3 treatment planned for four quadrants of SRP were enrolled in this pilot study. The range in patient age in this study was 35–75 years without a current history of smoking, diabetes, and/or any immunosuppressive disorders. After informed consent was signed, a saliva sample was taken from the patients and submitted for oral DNA analysis. The patients then had oral hygiene instruction demonstrated and were given the StellaLife Vega Oral Recovery Kit. Patients were instructed to use the rinse three times a day for 60 seconds, three pumps of the spray sublingually (under the tongue) three times a day, and then, with a clean Q-tip, rub the gel on the buccal and palatal/lingual gingival tissue three times a day.
Oral DNA test
The oral DNA test (OraVital Biofilm Diagnostics Microbiology Lab) received measured specific types of bacterial levels from five different areas of the mouth per
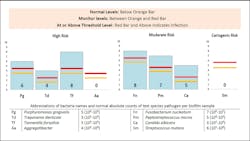
Genomic DNA is extracted from the submitted sample for eight oral species associated with periodontal disease, caries, and candidiasis. The bacteria are tested by quantitative polymerase chain reaction (qPCR) using an absolute quantification method, and readings are interpreted against the standard curve for each pathogen obtained from the amplification of related plasmid DNA.
Red and orange threshold levels are based on current literature and reported in log copies per sample (figure 1). Bacterial counts above the red line mean infection, between the red and orange lines mean monitor the patient for progression, and below the orange line indicate within acceptable normal range.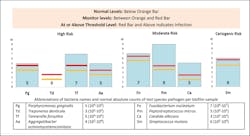
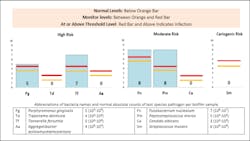
Overall bacterial counts were recorded and compared prior to (figure 2) and after therapeutic intervention (figure 3) and reported as percent reduction, no change, or percent increase in colony counts.
Results and conclusions
Ten patients with generalized moderate to chronic periodontal disease scheduled
References
- Tsay SV, Bartoces M, Gouin K, Kabbani S, Hicks LA. Antibiotic prescriptions associated with COVID-19 outpatient visits among Medicare beneficiaries, April 2020 to April 2021. JAMA. 2022;327(20):2018-2019. doi:10.1001/jama.2022.5471
- Lee S. NIH awards $2.4. million grant to UT Health San Antonio and ADA Science & Research Institute to study responsible antibiotic use. UT Health San Antonio. April 27, 2022. https://news.uthscsa.edu/nih-awards-2-4-million-grant-to-ut-health-san-antonio-and-ada-science-research-institute-to-study-responsible-antibiotic-use/
- Kapoor A, Malhotra R, Grover V, Grover D. Systemic antibiotic therapy in periodontics. Dent Res J (Isfahan). 2012;9(5):505-515. doi:10.4103/1735-3327.104866
- May B. More selective antibiotic shows promise for difficile infection. Medscape. May 6, 2022. https://www.medscape.com/viewarticle/973563
- Angelucci F, Cechova K, Amlerova J, Hort J. Antibiotics, gut microbiota, and Alzheimer’s disease. J Neuroinflammation. 2019;16(1):108. doi:10.1186/s12974-019-1494-4
- Lee CR, Cho IH, Jeong BC, Lee SH. Strategies to minimize antibiotic resistance. Int J Environ Res Public Health. 2013;10(9):4274-4305. doi:10.3390/ijerph10094274
- Zhou P, Chrepa V, Karoussis I, Pikos MA, Kotsakis GA. Cytocompatibility properties of an herbal compound solution support in vitro wound healing. Front Physiol. 2021;12:340. doi:3389/fphys.2021.653661
- Fujioka-Kobayashi M, Schaller B, Pikos MA, Sculean A, Miron RJ. Cytotoxicity and gene expression changes of a novel homeopathic antiseptic oral rinse in comparison to chlorhexidine in gingival fibroblasts. Materials (Basel). 2020;13(14):3190. doi:3390/ma13143190
- Batra C, Alalshaikh M, Gregory RL, Windsor LJ, Blanchard SB, Hamada Y. An in vitro comparison of four antibacterial agents with and without nicotine and their effects on human gingival fibroblasts. J Periodontol. 2022;93(2):e24-e33. doi:1002/JPER.21-0262
- IBM Micromedex. Chlorhexidine (oral route). Side effects. Mayo Clinic. Updated February 1, 2022. https://www.mayoclinic.org/drugs-supplements/chlorhexidine-oral-route/side-effects/drg-20068551
- Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: framework and proposal of a new classification and case definition. J Periodontol. 2018;89(Suppl 1):S159-S172. doi:10.1002/JPER.18-0006. Erratum in: J Periodontol. 2018;89(12):1475. doi:10.1002/jper.10239
About the Author

Scott Froum, DDS
Scott Froum, DDS, a graduate of the State University of New York, Stony Brook School of Dental Medicine (SUNY), is a periodontist in private practice in New York City. He is the editorial director of Perio-Implant Advisory and serves on the Dental Economics advisory board. Dr. Froum is a volunteer professor in the postgraduate periodontal program at SUNY, is a trained naturopath, and is the scientific director of Meraki Integrative Functional Wellness Center. Contact him at drscottfroum.com.
Read Dr. Froum's DE Editorial Advisory Board profile here.