Cortisol, stress, and your dental patient
Key Highlights
- Cortisol dysregulation drives inflammation, delays healing, and directly impacts periodontal and implant outcomes.
- Distinct stress patterns (“wired,” “tired and wired,” “tired”) present with unique symptoms that influence dental care and patient behavior.
- Strategic scheduling, stress-reduction techniques, and targeted support can improve clinical outcomes and patient experience.

Stress is no longer a vague psychosocial concept relegated to mental health disciplines—it is a measurable, biologically mediated phenomenon with direct implications for oral and systemic health. Central to this response is cortisol, the primary glucocorticoid hormone produced by the adrenal cortex under hypothalamic--pituitary--adrenal (HPA) axis regulation.
For dental professionals, appreciating how cortisol fluctuates—and how dysregulation manifests clinically—is critical. From impaired wound healing and increased periodontal breakdown to altered pain perception and patient behavior, cortisol serves as a physiologic bridge between systemic stress and oral disease.1
This article explores cortisol’s biologic and psychologic roles, clinical cortisol patterns, and practical strategies for managing patients with stress--related dysregulation
Biologic/psychologic stress and cortisol
The hormonal cascade of stress
Cortisol is not an isolated hormone—it orchestrates a wide systemic response. Under stress, the following physiologic changes occur2:
- Cortisol
- Adrenaline and glucagon
- Free fatty acids
- Prolactin
- Reverse T3 (metabolic downregulation)
- Body fat deposition
- Muscle mass
Clinically, this translates to:
- Impaired immune function → increased periodontal inflammation
- Delayed wound healing → compromised surgical outcomes
- Altered glucose metabolism → worsened glycemic control
- Catabolic tissue effects → soft tissue breakdown
For dental care providers, these changes are not theoretical—they directly affect implant integration, graft success, and peri--implant tissue stability. In fact, cortisol levels in peri--implant sulcus fluid were linearly correlated with probing depth, with evidence suggesting this relationship may be independent of hyperglycemia. Depression emerged as the most significant for chronically stressed patients and was associated with peri--implantitis. The thought is that cortisol level induces peri--implantitis via inflammation by modulating cytokine expression effects.3
Additional reading: The circadian rhythm and dentistry: Is there a connection?
Cortisol awakening response
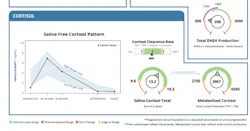
The cortisol awakening response (CAR) represents a physiologic surge in cortisol within 30–60 minutes of waking. In healthy individuals, this rise is typically 50%–160% above baseline, preparing the body for metabolic and cognitive demands. Figure 1 shows the result of a Dried Urine Test for Comprehensive Hormones (DUTCH) measuring cortisol throughout a patient’s day. This diurnal cortisol pattern is supposed to increase in the morning to its highest elevated point 30 minutes to one hour after waking, and then slowly decrease throughout the day until the lowest levels, which are supposed to be around bedtime.
The blunted or “flat-lined CAR”
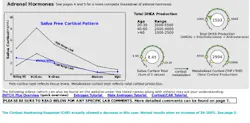
A blunted CAR suggests that the patient wakes up and does not get that burst of energy and can remain tired throughout the day. This can be the result of (figure 2):
- Total cortisol production is reduced.
- DHEA levels may also be suboptimal.
- HPA axis dysregulation
- Chronic stress adaptation (not acute stress)
- Reduced physiologic resilience
In dental settings, these patients often present with: fatigue, reduced healing capacity, increased inflammation despite adequate hygiene, heightened pain sensitivity.
3 cortisol profiles and their dental clinical significance
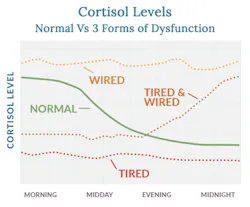
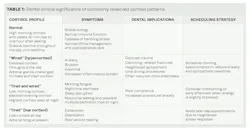
Patients may present as “wired,” “tired and wired,” or “tired,” (figure 3) each associated with distinct symptoms and clinical considerations (table 1).
Supporting dysregulated cortisol profiles
Adaptogenic and nutritional support
Based on the provided data and clinical literature:
- Astragalus → immune modulation
- Rhodiola → improves stress resilience
- Siberian/Panax ginseng → enhances energy and cognitive function
- Cordyceps → supports mitochondrial activity
- Passionflower → GABA modulation, reduces anxiety
- Panax Ginseng → mood stabilization, methylation support
- Relora (Magnolia + Phellodendron) → reduces cortisol and perceived stress
- 5-HTP → serotonin precursor, improves sleep and mood
These interventions can be particularly beneficial in patients exhibiting low cortisol or dysregulated diurnal rhythms, improving both systemic health and oral outcomes.
Lifestyle techniques to lower stress
Schneider et al. (American Journal of Cardiology, 2006) demonstrated that stress reduction interventions, including cognitive behavioral therapy (CBT), significantly reduce cardiovascular events.
For dental professionals, this reinforces both the importance of recognizing chronic stress patterns and referring patients for behavioral therapy when appropriate.
- Exercise and BDNF.4 Exercise increases brain--derived neurotrophic factor (BDNF) which enhances neuroplasticity, reduces stress, improves mood. This has direct implications for: pain tolerance, anxiety reduction, and postoperative recovery.
- Vagal nerve stimulation and autonomic balance.5 Vagal stimulation promotes parasympathetic activation, reduces cortisol, and improves heart rate variability. Clinically relevant tools include breathing techniques and wearable vagal stimulation devices.
- Music and neural regulation.6 Listening to or playing music reduces cortisol, enhances dopamine release, improves emotional regulation. In--office application can be playing calming music during procedures and patient--controlled audio environments.
- Social connection and emotional affection.7 Human connection reduces cortisol, increases oxytocin, enhances immune response. Patients with strong social networks consistently show better healing outcomes and lower inflammatory burden.
Actionable strategies for dental professionals
- Biologic stress management
• Identify cortisol patterns via history or testing.
• Schedule appointments strategically.
• Recommend adaptogens and nutritional support.
• Coordinate with physicians when needed.
- Psychologic stress management
• Screen for anxiety and chronic stress.
• Incorporate calming operatory environments.
• Encourage CBT or mental health referral.
• Use music, breathing, and vagal techniques.
- In-office protocol enhancements
• Longer appointment times for high--stress patients
• Clear communication to reduce uncertainty
• Minimize procedural pain triggers.
• Consider sedation strategies when appropriate.
Conclusion
Chronic psychological stress is no longer viewed as a purely behavioral phenomenon—it is a biologically mediated process with direct implications for both neural integrity and cardiovascular risk.8 Activation of the hypothalamic–pituitary–adrenal (HPA) axis leads to sustained elevations in cortisol and catecholamines, which, over time, alter hippocampal and prefrontal cortex function while promoting amygdala hyperreactivity.9 This neuroendocrine imbalance impairs executive function, decision-making, and emotional regulation—factors that are highly relevant to patient compliance and health behaviors.
From a periodontal and systemic perspective, prolonged cortisol exposure contributes to immune dysregulation, increased pro-inflammatory cytokine release, and endothelial dysfunction.10 Recognizing stress phenotypes—whether hypercortisolemic or “burned out” with flattened diurnal rhythms—can inform not only behavioral counseling but also appointment timing, perioperative management, and interdisciplinary referral. Incorporating stress assessment into routine care, even through targeted questioning or salivary biomarkers, positions the dental office as a frontline screening environment for systemic disease. In this context, managing periodontal inflammation is not simply about preserving dentition—it becomes part of a broader strategy to mitigate neuroinflammatory and cardiovascular sequelae associated with chronic stress.
Editor's note: This article appeared in the May 2026 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
References
- Decker AM, Kapila YL, Wang HL. The psychobiological links between chronic stress-related diseases, periodontal/peri-implant diseases, and wound healing. Periodontol 2000. 2021;87(1):94-106. doi:10.1111/prd.12381
- Kivimäki M, Bartolomucci A, Kawachi I. The multiple roles of life stress in metabolic disorders. Nat Rev Endocrinol. 2023;19(1):10-27. doi:10.1038/s41574-022-00746-8
- Chang YL, Lin GM, Lin SY, et al. Evidence for the association between psychological stress and peri-implant health among middle-aged and elderly adults: a systemic review. World J Clin Cases. 2025;13(23):105762. doi:10.12998/wjcc.v13.i23.105762
- Rico-González M, González-Devesa D, Gómez-Carmona CD, Moreno-Villanueva A. Exercise as modulator of brain-derived neurotrophic factor (BDNF) in children: a systematic review of randomized controlled trials. Life (Basel). 2025;15(7):1147. doi:10.3390/life15071147
- Bremner JD, Gurel NZ, Wittbrodt MT, et al. Application of noninvasive vagal nerve stimulation to stress-related psychiatric disorders. J Pers Med. 2020;10(3):119. doi:10.3390/jpm10030119
- Thoma MV, La Marca R, Brönnimann R, Finkel L, Ehlert U, Nater UM. The effect of music on the human stress response. PLoS One. 2013;8(8):e70156. doi:10.1371/journal.pone.0070156
- Bremner JD, Gurel NZ, Wittbrodt MT, et al. Application of noninvasive vagal nerve stimulation to stress-related psychiatric disorders. J Pers Med. 2020;10(3):119. doi:10.3390/jpm10030119
- Vaccarino V, Shah AJ, Mehta PK, et al. Brain-heart connections in stress and cardiovascular disease: implications for the cardiac patient. Atherosclerosis. 2021;328:74-82. doi:10.1016/j.atherosclerosis.2021.05.020
- Tawakol A, Ishai A, Takx RA, et al. Relation between resting amygdalar activity and cardiovascular events: a longitudinal and cohort study. Lancet. 2017;389(10071):834-845. doi:10.1016/S0140-6736(16)31714-7. Erratum in: Lancet. 2017;389(10071):804. doi:10.1016/S0140-6736(17)30082-X. Erratum in: Lancet. 2017;389(10071):804. doi:10.1016/S0140-6736(17)30344-6
- Macrì M, D'Albis G, D'Albis V, et al. Periodontal health and its relationship with psychological stress: a cross-sectional study. J Clin Med. 2024;13(10):2942. doi:10.3390/jcm13102942
- Villafuerte KRV, Palucci Vieira LH, Santos KO, Rivero-Contreras E, Lourenço AG, Motta ACF. Psychological stress reduces the effectiveness of periodontal treatment: a systematic review. J Clin Med. 2025;14(5):1680. doi:10.3390/jcm14051680
About the Author

Scott Froum, DDS
Scott Froum, DDS, a graduate of the State University of New York, Stony Brook School of Dental Medicine (SUNY), is a periodontist in private practice in New York City. He is the editorial director of Perio-Implant Advisory and serves on the Dental Economics advisory board. Dr. Froum is a volunteer professor in the postgraduate periodontal program at SUNY, is a trained naturopath, and is the scientific director of Meraki Integrative Functional Wellness Center. Contact him at drscottfroum.com.
Read Dr. Froum's DE Editorial Advisory Board profile here.

Micaela Milano, MBA
Micaela Milano, MBA, is the owner and founder of Meraki Integrative, where she combines her extensive professional experience and passion for holistic health to deliver personalized, transformative care. Micaela holds an MBA in business, marketing, and management from Florida International University. In 2018, she founded the Meraki Initiative, dedicating herself to integrative wellness and client empowerment. A certified 200-hour yoga teacher, Reiki practitioner, and advanced holistic health coach, Micaela also holds certifications in angelic and crystal healing, bringing a deeply personal and spiritual dimension to her work.
Douglas Isaacs, MD
Douglas Isaacs, MD, is a board-certified physician in emergency medicine and emergency medical services (EMS) with over 20 years of experience in academic medicine and clinical leadership. A graduate of Cornell University Medical College, he completed dual residencies in internal medicine and emergency medicine, followed by a fellowship in emergency medical services. For the past five years, he has been deeply involved in regenerative and functional medicine, merging cutting-edge science with holistic patient care. Dr. Isaacs is the medical director of Meraki Integrative Wellness.