Improving the life cycle of teeth
Each month, Dr. Gordon Christensen answers a question from readers about everyday dentistry.
Q: When observing the recent ads and articles in dental journals and magazines, it is obvious that there is high emphasis on the techniques and concepts that are at the end of the life cycle of teeth. Even though All-on-X, full-mouth rehabilitation, implants, complex and heroic perio, and other topics are important and timely, it seems that more emphasis should be placed on research and clinical procedures on the other end of the cycle to prevent caries, periodontal disease, and malocclusion.
Is there something we can do to redirect dentistry toward an emphasis on increasing and effectively implementing revenue-producing preventive procedures?
A: You have expressed my favorite and most frustrating topic. Even though I am a prosthodontist and enjoy doing complex treatments, I know very well that when they are needed, the profession and the patients have failed. The following information traces the various stages of dental prevention and treatment as well as the products and ways dental disease can be stopped or at least slowed at each stage.
Oral health education programs
The main reason for any education on almost any topic is behavior change! At any stage of life, behavior change on preventive dentistry concepts can help reduce potential negative issues with caries, periodontal disease, and occlusal challenges. Influencing behavior change varies in direct relation to overall education, income, motivation, health, and other factors. “Effectiveness of oral health education programs: A systematic review” is a great resource on this topic.1 Details are in the reference.


Prenatal
Most mothers-to-be are not think-ing about their child’s teeth. However, research shows that mothers who have had preventive dentistry instruction during their pregnancy and postpartum period have children with fewer carious lesions than those without such instruction. Some communities with motivated dental societies, hospitals, civic groups, or other organizations have educational sessions for pregnant women that include ways to reduce or eliminate the well-known challenges facing their newborn, including the most frequent disease of childhood—dental caries.
Early childhood
From 8 to 33 months of age, various types of primary teeth erupt into a child’s mouth. This is an especially important time to incorporate preventive dentistry concepts. At least for the first few months of the child’s life, the mother is completely engrossed with infant care and feeding the child by bottle, breast, or both.
As teeth erupt causing the child to cry, there is a significant tendency for the caregiver to provide sweet liquids to calm the child. The resultant “bottle mouth” problem is rampant worldwide, especially in developing countries.
Eating solid foods at 7 or 8 months can be a challenge, and, again, foods containing sugar are often better accepted by the child. However, advise caregivers not to give these sugary foods to their children because it may lead to sugar addiction.
Gum brushing can start as soon as the child accepts it, and toothbrushing comes as soon as teeth appear.
The importance of a healthy early childhood diet, proper oral hygiene, acceptable professional care, and constant parental guidance on dental care is obvious. If done correctly and with proper professional use of fluoride, no or few carious lesions will be present, depending on whether community water is fluoridated. The child will learn to eat the proper foods and clean their mouth, which can continue to develop into optimal long-term preventive dental behavior.
Teenage years
During these years, the major challenge begins, as the known negative psychological characteristics of most teenagers are present. Oral hygiene can become less important for the teenager as major changes begin to occur in their life. Parents should try to keep teenagers on the same preventive dental procedures that they developed during childhood. If the parents have instilled good preventive procedures, the teenager will probably continue. If not, you know the result—new dental caries.
A small percentage of teenagers reject parental suggestions. In such cases, at least suggest the use of high-level fluoride-containing toothpastes, the use of which is not a major behavior change from using low 1,000 ppm fluoride-containing toothpastes. Colgate Prevident 5,000 Booster Plus used once daily is one of the most popular brands (figure 1). Fluoride in trays is even better if you think the patient will be compliant.

At this stage, orthodontics should be considered, if necessary, to improve esthetics and reduce occlusal problems later in life, but it does increase the potential for new caries.
Continue to encourage a proper diet and good oral hygiene—and good luck!
Young adulthood
A well-known dental hygiene advantage is now present. Mom and Dad probably are no longer paying for oral care, and the financial challenge the young adult feels can cause consciousness of the cost of dental neglect. The necessity of good oral preventive procedures to prevent the social stigma of decayed teeth and bad breath may become evident to the young adult. The standard suggestions for acceptable preventive dental care should continue to be emphasized by dentists, hygienists, assistants, and public health agencies.
Middle age
The emergence of periodontal disease is now present in at least 30% of your patients, and they don’t even know it’s there unless they are advised by their dental professionals.
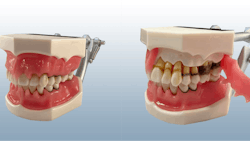
Hygienists and dentists can educate their patients by using models that show the stages of periodontal disease. Then, they can begin treatment at an early stage. Artificial intelligence is now being used to predict the progress of periodontal disease and will be even more advantageous for patient education.
Although many companies have periodontal disease models, Kilgore has one of the most impressive, convincing, and educational ones (figure 2). Patients can see what is happening to their oral bone and soft tissue when educated by you or your staff.

I suggest having these patients come in for professional dental services every two to three months instead of the standard six. Have your hygienists take responsibility for these patients by using conservative periodontal procedures. As your patients experience reduced periodontal disease, you’ll have increased practice revenue.
Senior years
Caries, periodontal disease, and occlusal challenges in senior citizens are well-known! These patients should be on frequent recare appointments and have optimum hygiene care. Apply 5,000 ppm fluoride in trays or toothpastes and instruct your patients on proper diet and oral hygiene. I strongly suggest advising seniors to use mechanical toothbrushes (figures 3 and 4).


Summary
Here, I have described the life cycle of human teeth. As each stage has been discussed, it is evident that if known preventive care is provided, reduction or even total prevention of caries, periodontal disease, and adverse occlusal situations is possible. Our goal as dental professionals should be to provide preventive education and preventive procedures at the earliest stage possible to allow use of human teeth throughout a lifetime. It is possible!


Editor's note: This article appeared in the June 2024 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
Reference
- Nakre PD, Harikiran AG. Effectiveness of oral health education programs: a systematic review. J Int Soc Prev Community Dent. 2013;3(2):103-115. doi:10.4103/2231-0762.127810
About the Author

Gordon J. Christensen, DDS, PhD, MSD
Gordon J. Christensen, DDS, PhD, MSD, is founder and CEO of Practical Clinical Courses and cofounder of Clinicians Report. His wife, Rella Christensen, PhD, is the cofounder. PCC is an international dental continuing education organization founded in 1981. Dr. Christensen is a practicing prosthodontist in Provo, Utah.