Why should teeth be removed?

Each month, Dr. Gordon Christensen answers a question from readers about everyday dentistry.
Q: I have been out of dental school for two years and have been pondering an important question that I see routinely in my patients. I worked for a corporation for 18 months; the group had different opinions about tooth removal than I was taught in dental school. Now, I’m having to make my own conclusions about when tooth removal is a viable alternative. What tooth characteristics do you use when deciding when to remove teeth?
A: I’ll share information that will help you know when to remove (or keep) teeth along with detailed procedures and materials to successfully build up broken-down teeth.
As you know, there are numerous factors that relate to your question:
- Can the tooth be restored?
- What is the patient’s financial situation?
- What is the pulpal status of the tooth? Is endodontic treatment feasible?
- How much of the coronal tooth structure is still present?
- Does the patient want to keep the tooth (or teeth)?
- Is the bone support adequate?
- What is the periodontal condition?
- What is the caries activity?
- What is the status of occlusion and/or bruxism?
- How is the patient’s oral hygiene?
- What is the patient’s diet?
- How is the patient’s overall health?
- What’s the patient’s age?
Assuming none of these factors or a combination of them mandates tooth removal, what characteristics should be present to allow tooth retention?
You may also be interested in ... Does that tooth really need endo?
Is the patient serious about keeping their teeth?
I don’t suggest trying to convince a doubting patient to keep their teeth. Provide proven information about the undesirable conditions following tooth removal as well as the few desirable ones. Be logical and factual as you educate your patient and let them have a part in making the decision. Make sure you have adequate informed consent signed by the patient. For tooth retention to be successful, significant commitment and behavior changes are required on the part of the patient.
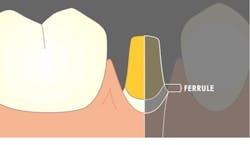
Is there enough supra-bone tooth structure remaining for a ferrule?
Usually, 2.0 mm of tooth structure (or 1.5 mm under certain circumstances) must be present to make an adequate ferrule (figure 1). If adequate tooth structure is not present, orthodontic extrusion, although seldom accomplished, could be done to allow space for the ferrules (if the root has adequate length).
Do other broken-down teeth in the same patient require similar treatment?
In patients requiring many tooth buildups, there are negative factors to consider. Buildups and crowns require optimum oral hygiene. If the patient has not practiced adequate oral hygiene, they probably won’t start now. The patient must be committed to changing their oral hygiene behavior and possibly their diet.
The financial investment of multiple buildups, some endodontic treatment, posts and cores, and crowns may be impossible for the patient to manage. If financial help is available, this may not be an impediment.
You may also be interested in ... How long do dental restorations last?
Do you feel comfortable placing tooth buildups?
Unacceptable tooth buildups are a major reason for crown failure. It has been my observation that many dentists could do more adequate tooth buildups.
The following steps provide tooth buildups with optimum crown retention, cariostatic characteristics, and good longevity of the final restoration. Most of the statements below have been researched by Clinicians Report Foundation (CR). Details are available on the CR website.
Technique for tooth buildups
Buildups accomplished with this technique are strong, retentive, cariostatic, well proven, and will provide excellent service if the patient has acceptable oral hygiene.
- Make optimum retention of the buildup material to the remaining tooth structure. What are the best methods to accomplish this? It is not bonding agents alone. These materials produce initial bond to dentin and tooth desensitization, but the retention soon depreciates with unavoidable contact with hot and cold foods.
Make grooves, channels, and small indentations for retention in the remaining tooth structure with one-half or one-quarter round burs. Place undercuts in the remaining tooth structure where old restorations have been removed.
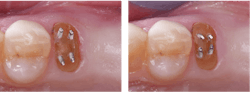
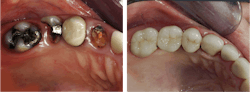
If half or more of the coronal portion of the prep is gone, use retentive pins. Use pure titanium pins placed nonparallel to one another and bent over to the center of the buildup. These provide optimum retention of composite to remaining tooth structure (figures 2 and 3). Avoid stainless steel pins; they have been proven to cause tooth cracks and occasional discoloration. - Make sure you have 2.0 mm of tooth structure ferrule around the prep coronal to the margins.
- Use two one-minute applications of glutaraldehyde-containing material for disinfection and desensitization of the prep (figure 4).
- Use composite materials specifically manufactured for tooth buildup (figure 5). Conventional restorative composite resin costs significantly more and doesn’t have any more desirable characteristics.
- If possible, build the tooth preparation with at least 4.0 mm of axial wall length from the cervical prep margin to the occlusal table, while still allowing 2.0 mm of occlusal reduction. If there is not enough tooth structure for 4.0 mm or more of axial length, such as mandibular second molars, make the prep as parallel as possible and place parallel facial-lingual and mesial-distal grooves in it. Before crown cementation, roughen the axial walls of the tooth prep and the crown internally.
- Produce 20 degrees or less axial deviation of the prep from the long axis of the tooth.
- Create basic anatomy in the occlusal table to allow the technician to make optimum occlusal anatomy in the crown.
- When seating the crown, use a cariostatic cement. Resin cements do not have cariostatic properties. Resin-modified glass ionomer (such as RelyX Luting Plus or GC FujiCEM Evolve) or conventional glass ionomer (such as Fuji 1 or Ketac Cem) are recommended (figure 6).



Summary
There’s no restorative substitute with the same positive characteristics as a natural tooth. Both the doctor and patient should give careful consideration to the removal of any natural tooth. Once teeth are removed, it’s final; they can’t be replaced. Decisions about tooth removal are difficult to make because there are so many things to consider. I suggest that dentists provide detailed informed consent for patients that allows them to make the best decisions for their situation. Saving broken-down teeth is possible when using proper, proven retentive buildups and the restorative procedures described in this article.
Editor's note: This article appeared in the November 2023 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
Author’s note: The following educational materials from Practical Clinical Courses offer further resources on this topic.
One-hour videos:
- Strong, Comfortable, Esthetic Rehabilitations with Zirconia (Item #V1942)
- Foolproof, Fast Single Crown Restoration (Item #V1980)
Two-day hands-on course in Utah:
- Faster, Easier, Higher Quality Dentistry with Dr. Gordon Christensen
- Fixed Prosthodontics Simplified with Dr. Gordon Christensen
- Simplifying Complex Treatment with Dr. Gordon Christensen
For more information, visit the Practical Clinical Courses website or call (800) 223-6569.
Gordon J. Christensen, DDS, PhD, MSD, is a practicing prosthodontist in Provo, Utah. He is the founder and CEO of Practical Clinical Courses, an international continuing education organization founded in 1981 for dental professionals. Dr. Christensen is cofounder (with his wife, Rella Christensen, PhD, RDH) and CEO of Clinicians Report.
About the Author

Gordon J. Christensen, DDS, PhD, MSD
Gordon J. Christensen, DDS, PhD, MSD, is founder and CEO of Practical Clinical Courses and cofounder of Clinicians Report. His wife, Rella Christensen, PhD, is the cofounder. PCC is an international dental continuing education organization founded in 1981. Dr. Christensen is a practicing prosthodontist in Provo, Utah.