Calculating the ROI of dental sleep medicine

Though obstructive sleep apnea (OSA) was discovered in 1965, it took another 20 years or so before savvy dentists began to contribute to the diagnosis and treatment of this disorder.1-2
Odds are, you’ve attended a seminar that talked about treating sleep apnea, just like tens of thousands of your peers. But despite all this training, it’s estimated that over 80% of those with OSA remain undiagnosed and/or untreated.3-8
The opportunity for dentists to build profitable businesses that provide this simple, life-altering treatment to the undiagnosed is immense. We have an opportunity to look through the lens of ROI: return on investment.
Dental sleep therapy: It's a math problem
Any new specialty, medical device, or procedure comes with a price tag (training, education, equipment, staffing, legal aspects)—so, when it comes to dental sleep medicine, what are practice owners seeing from the perspective of a return?
Barriers to ROI: Critical success factors
The biggest barrier to positive ROI is simple: it’s in the setup. Most dentists get a cursory picture of how to successfully implement and bill for sleep apnea treatments, but that usually isn’t enough. Why? Without knowing how to handle insurance claims for sleep disorder appliances, the dentist makes a half-hearted attempt at delegating billing to an untrained employee, only to receive a reimbursement somewhere between $0 and $1,200.9-13
Case study: Dr. Jay Neuhaus
Meet Dr. Jay Neuhaus. Dr. Neuhaus practices dental sleep medicine in Manhattan. He currently works just two days per month seeing patients in his practice. Here’s his report:
“Today, I rent two operatories two days a month, and other than my beautiful wife, my only other payroll is a chairside assistant who only gets paid for two days a month. With this low overhead, we’re able to help 15–20 patients a month with an average net of $4,000 an appliance.”
Dr. Neuhaus is seeing 20 patients per month x 12 months x $4,000 per appliance. That’s an annual gross of just under $1 million. Dr. Neuhaus isn’t the only dentist treating sleep apnea who has enjoyed results like these.
A scalable model for success
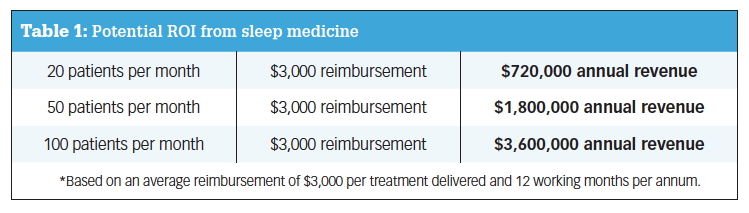
Based on the data we’ve collected from working with hundreds of dentists treating sleep apnea, Table 1 shows what we’ve learned about generating potential ROI.

For there to be a return, there must be an investment. In the case of treating obstructive sleep apnea, here are five key components of that overall investment:
- Sleep coordinator salary
- Legal entity creation
- Billing software or vendor partner
- Training and education for both the doctor, administrative staff, and hygienists
- Continuing education or diplomate training
This is not an exhaustive list, but it does capture some of the key success factors that are critical for dentists who are exploring dental sleep medicine.
When it comes to training and education, thoroughness is the watchword. Sleep courses promising a simple, easy way into dental sleep medicine have been around for decades.
So why aren’t there more success stories in dental sleep medicine?
It comes down to focus and intention. Based on the “general wisdom” presented in sleep courses, successful sleep dentists might see only one to two patients per month. Some might go without seeing a single sleep treatment patient for months. They might offer the solution offhandedly if or when the conversation arises with a patient who’s already in their chair for a general checkup or other common treatment. These dentists simply aren’t going all-in on dental sleep medicine. And that’s OK if you’re not trying to build a practice that centers on treating sleep disorders.
Consider overhead
A general practice comes with a lot of overhead: operatories, equipment, staffing, insurance companies, not to mention competitors willing to race to the bottom on price. Dental sleep medicine doesn’t demand we continue that paradigm. In fact, dental sleep practices have far lower overhead. This is due specifically to the simplicity of the treatment. There is no need for a large staff, expensive equipment, or a heavy dependence on volume of procedures delivered (given the relatively low billable return on preventive maintenance). So, at $3,000 per appliance in gross revenue and fewer operational costs contributing to overhead, this return is a much more efficient result.
Leveraging time as a factor
The longer you’re in practice as a dental sleep professional, the more your initial investment continues to bear fruit. What is the best way to maximize profits from dental sleep medicine? Begin the journey early in your dental career. As with any treatment, your mileage may vary. Success factors beyond those that we’ve captured here should not go unmentioned. Your motivation and constructive action as a health-care professional—a health-care entrepreneur—has perhaps as much to do with your ROI as implementing the correct strategies and standard operating procedures.
ROI: Beyond the financial benefits of dental sleep medicine
Many practicing dentists find sleep disorder treatment later in their career, and they, too, have been able to create significant new success. Dr. Dana Blalock wanted to transition to sleep dentistry from restorative dentistry. And, after more than three decades in practice, she did just that:
“As I began to see more sleep patients, I also realized how rewarding it is to treat these patients, improve their sleep, improve their health and overall well-being. How often does a dental patient tell you how much they ‘hate the dentist’? After 36 years of practicing dentistry, I don’t have to hear that from my sleep patients! They are so happy to get this help and special treatment—they love us!”
Additionally, Dr. Blalock loves how there’s less physical stress on her body as the dentist. For many practitioners, this is one of the “hidden costs” of doing the job. For dentists who are experiencing the normal aches and pains associated with aging but who are not yet ready to retire, dental sleep medicine can potentially save some of that strain on the body.
Author’s note: The two dental sleep practitioners quoted have both completed the Dental Sleep MBA program by the International Academy of Sleep (IAOS). As a provider of PACE-approved continuing education programs for dentists, IAOS helps dentists create profitable sleep businesses. From business to clinical to patient communication, IAOS provides the tools and resources needed for a dentist to become the go-to sleep expert in their area. We invite Dental Economics readers to learn more about dental sleep medicine by attending one of our upcoming Sleep Practice Blueprint events that goes into much greater detail on both treating OSA as a dentist and how to set up a practice dedicated to dental sleep medicine. Learn more and get dates for our upcoming live events at iaos.com/live.
Editor's note: This article appeared in the November 2022 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
References
1. Dement WC. The study of human sleep: a historical perspective. Thorax. 1998;53(Suppl 3):S2-S7. https://thorax.bmj.com/content/thoraxjnl/53/suppl_3/S2.full.pdf
2. Quan SF, Schmidt-Nowara W. The role of dentists in the diagnosis and treatment of obstructive sleep apnea: consensus and controversy. J Clin Sleep Med. 2017;13(10):1117-1119. doi:10.5664/jcsm.6748
3. Chung F, Liao P, Singh M, Kobah S, Elsaid H. What is the proportion of undiagnosed obstructive sleep apnea in a surgical population? Chest J. 2010;138(4):781A. doi:10.1378/chest.9993
4. Ikpeze T. Sleep apnea treatments. SleepApnea. Updated September 29, 2022. https://www.sleepapnea.org/learn/sleep-apnea-information-clinicians/
5. Santilli M, Manciocchi E, D’Addazio G, et al. Prevalence of obstructive sleep apnea syndrome: a single-center retrospective study. Int J Environ Res Public Health. 2021; 18(19):10277. doi:10.3390/ijerph181910277
6. Lee W, Nagubadi S, Kryger MH, Mokhlesi B. Epidemiology of obstructive sleep apnea: a population-based perspective. Expert Rev Respir Med. 2008;2(3):349-364. doi:10.1586/17476348.2.3.349
7. What are the effects of sleep apnea? Cleveland Clinic. Reviewed March 3, 2020. https://my.clevelandclinic.org/health/diseases/8718-sleep-apnea
8. American Osteopathic Association. Up to 15 percent of children have sleep apnea, yet 90 percent go undiagnosed. February 12, 2019. Accessed July 29, 2022. https://medicalxpress.com/news/2019-02-percent-children-apnea-undiagnosed.html
9. Home sleep apnea tests. American Academy of Dental Sleep Medicine. Accessed July 29, 2022. https://www.aadsm.org/home_sleep_apnea_tests.php
10. What does Medicare pay for E0486? (oral appliance to treat OSA). NiermanPM. Accessed July 29, 2022. https://help.niermanpm.com/knowledge/what-does-medicare-pay-for-e0486-oral-appliance-to-treat-osa
11. Data on file. International Academy of Sleep. 2022.
12. Sleep services 2021 vs. 2022 national payment comparison revised. American Academy of Sleep Medicine. Accessed July 29, 2022. https://j2vjt3dnbra3ps7ll1clb4q2-wpengine.netdna-ssl.com/wp-content/uploads/2021/11/sleep-payment-RVU-comparison-2021-2022.pdf
13. Rotenberg BW, Murariu D, Pang KP. Trends in CPAP adherence over twenty years of data collection: a flattened curve. J Otolaryngol Head Neck Surg. 2016;45(1):43. doi:10.1186/s40463-016-0156-0
About the Author

{kind=link}
Avi Weisfogel, DDS
Avi Weisfogel, DDS, is the CEO and founder of International Academy of Sleep (IAOS). As a “recovering dentist,” Dr. Weisfogel’s life and career have been transformed through his journey from general dentistry into the mastery of dental sleep medicine. Through his work in IAOS, he and his team help dentists create profitable sleep businesses. From business to clinical to patient communication, IAOS provides the tools and resources dentists need to become the go-to sleep expert in their area.
Updated October 6, 2022