Whole-person care for vulnerable patients: The value of medical-dental integration

Many in the health-care industry hear about integrating medical and behavioral health, but rarely do they discuss the importance of including dental in that paradigm. They forget that the mouth is part of the body, and to be truly healthy, one needs a healthy mouth. After all, oral diseases affect close to four billion people worldwide.1
Poor oral health can lead to tooth loss, untreated caries, and periodontal disease, which contribute to adverse health outcomes and high-cost preventable emergency room visits.2 People who are dually eligible for Medicare and Medicaid—primarily low-income seniors—are substantially more likely than other Medicare enrollees to face vision and dental problems.3
This dual-eligible population is five times more likely to have a disability and twice as likely to be hospitalized or die than their nondual counterparts. With complex conditions, they also have significantly worse outcomes,4 face greater social and financial challenges,5 and have less access to high-quality care.6
For most people, oral health care in the US is neither easy to obtain nor equitable. With a focus on restorative care and an outdated reimbursement system, dental care delivery in the US is ripe for transformation. Medical-dental integration (MDI) is a key path forward, particularly when addressing care and outcomes for those dually eligible.
What is MDI?
Also called interprofessional practice, MDI is rooted in science that shows addressing health issues holistically—not just oral care at the dental office and physical care at the medical office—improves outcomes and increases access to care for vulnerable populations.
Related articles
Driving medical-dental integration with telehealth technology
Medical and dental data integration: How can this become a reality?
We know dual eligible populations have complex needs: 41% have at least one mental health diagnosis, nearly half receive long-term care services and supports, and 60% have multiple conditions.7 They are also significantly less likely to have access to integrated care models that effectively close preventive care and disease management gaps.
The relationship between medical and dental is not in question, nor are the care inequities among dual-eligible populations with multiple comorbidities and medications. Despite clear medical need, patients with severe and persistent mental illness often lack access to dental care. Patients living in nursing homes or assisted facilities often arrive with poor oral health that may have already compromised their recovery.
The separation of medical and dental systems disproportionately burdens vulnerable populations—low-income people, people of color, people with disabilities, rural dwellers, and formerly incarcerated people are all more likely to suffer from dental disease and pain and to report difficulty gaining access to care.8
Enter integrated care delivery to effectively improve access and outcomes
MDI means helping patients get the care they need where they already receive support, creating a system that enables coordination and collaboration among a variety of providers regardless of physical location. It already happens in a number of pilot programs across the country, adding oral health screenings to well-child visits, enabling dental care providers to check insulin levels, using telehealth to connect providers from multiple disciplines with a single patient, and more.
Opportunities exist and have been successful adding oral health risk assessment and dental hygiene education into primary care visits, inpatient hospital wards, and many federally qualified health centers (FQHCs). For example, CareQuest Institute for Oral Health Improvement launched a pilot program in Massachusetts, the COVID-19 Oral Health Recovery and Transformation (COHRT) Learning Community.9 COHRT focused on teledentistry in oral health disease prevention, minimally invasive care, and integrated and personalized treatment. Providers had tools including monthly assistance calls, access to subject matter experts, and a private virtual learning environment that encouraged peer interaction, which enabled participants to identify concerns and strategies to mitigate them.
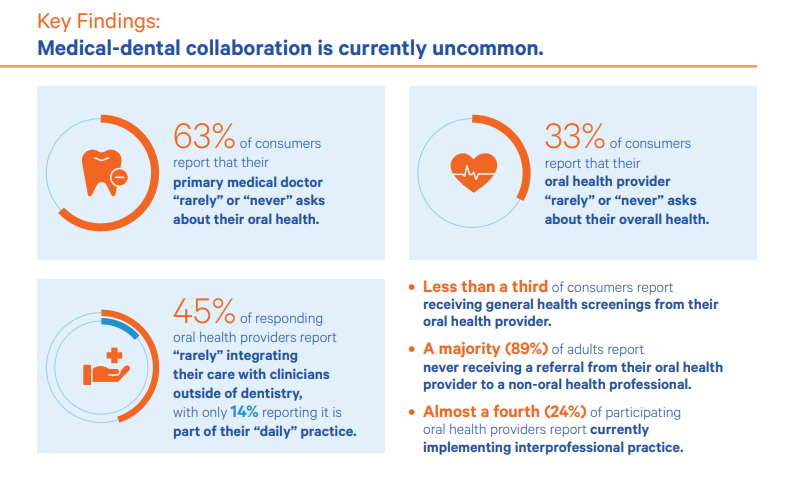
Yet overall, this is uncommon. CareQuest data shows consumers rarely are asked about their oral health at their primary care visits or about their medical health at their dental visits.10 And 45% of oral health providers report “rarely” integrating care with nondental clinicians (figure 1).10 Still, providers and care teams report higher satisfaction when using personalized planning.

{kind=link}
Lack of medical-dental collaboration
Recent data indicates providers are responsive to an integrated process, desire better screening and referral processes by interprofessional practices, and favor improved communication.9 What’s more, evidence suggests care providers have effectively improved quality and earned increased financial bonuses. Operations and care team salaries are also more stable, especially when providers are affiliated with a group network or dental service organizations operating within an integrated and value-over-volume financial structure.
What is the value of MDI?
Dually eligible beneficiaries account for one-third of total expenditures for both Medicare and Medicaid even though the percent of total enrollees who are dually eligible is 15% and 20%, respectively.7 These are high users of high-cost care, making them the right group for MDI opportunities that deal directly with case management, outreach, and the management of members’ oral health in the prevention or control of underlying health conditions.
Personalized, integrated care plans effectively decrease the number of emergency department visits, reduce overall health-care expenditures, and are well received by network providers. MDI can also indirectly drive significant cost saving by addressing undiagnosed systemic disease earlier and enhancing chronic disease management. Yearly savings could reach as high as $100 million if screenings for diabetes, high blood pressure, and high cholesterol occurred during dental care visits, according to the CDC.11
For example, past preventive periodontal services among Medicaid-enrolled adults with diabetes could save roughly 13% of overall costs and an even more startling 48% for inpatient costs.12 Another study shows $515 to $1,718 per member per year cost savings when patients with diabetes, coronary artery disease (CAD), or both had at least one preventive dental visit per year.13
For every 1% increase in patients receiving dental services, the proportion of diabetes patients with uncontrolled diabetes declined by 0.2% for the patient population seen at FQHCs.14 An American Dental Association study also points to significantly greater use of preventive and disease management services among patients ages 65 and older getting dental treatment at a clinic specifically designed around MDI.15
A healthier mouth and body, as well as preservation of tooth and gum tissue, can also lead to longer lasting dental restorations and improved surgical outcomes.
What needs to change for MDI?
Several challenges exist. Some can be solved among plans, some among providers and patients, and some among policymakers. These include issues with interoperability, benefit design, consistent networks, greater case management, and education.
Health information technology (HIT): The use of health information exchanges and development of common data and language between medicine and dentistry, among other HIT solutions to integrate medical and dental records, will be crucial for long-term adoption of interprofessional strategies. In addition, broader adoption of technology in dentistry can help achieve goals related to better outcomes, shorter appointment processes, and easier opportunities for education and knowledge development.
The separation of medical and dental systems disproportionately burdens vulnerable populations—low income people, people of color, people with disabilities, rural dwellers, and formerly incarcerated people are all more likely to suffer from dental disease and pain.
One of those technological advancements is telehealth/teledentistry. Synchronous telehealth visits involve real-time communication via video, phone, and chat between providers and patients. These types of virtual visits enable integrated, interprofessional care without being geographic- or location-specific. Providers can arrange for a more holistic experience by including interaction with both medical and dental care teams via telehealth to comprehensively meet the needs of patients, particularly those with mobility issues.
Asynchronous telehealth, on the other hand, refers providers uploading data for review with other specialists at another time. Primary care teams, especially those within integrated systems, are more likely to leverage telehealth for consultations with off-site specialists (cardiology, dermatology, etc.), and adding dental providers only expands access and improves overall outcomes. What’s more, this can work the other way around—dental providers can also offer virtual consults with medical providers, which further cements the dental provider’s essential role as part of the interdisciplinary health-care team.
However, to be most effective, telehealth and all care provided need to function within an infrastructure that supports every type of care in the same environment. Interoperability is vital; electronic medical and dental records are as separate as the care systems themselves. There have been important standards updates to support dental data exchange, but there’s a long road ahead. At a national level, these systems should facilitate efficient transfer of information, not just to improve patient care but also to improve data collection and measurement. The current standard forcing practices to rely on manual processes or time-intensive workarounds to communicate across disciplines is unsustainable.
Benefit design and networks: We need cohesive dental benefit design between both Medicaid and Medicare to not only support dual-eligible members, but also to reduce friction for all members, providers, and administrators. In short, the benefit design must be comprehensive and integrated across Medicaid and Medicare benefit structures while not limiting the beneficiary to oral health resources that have a direct correlation to improved health and lower cost of care.
Benefit designs also need financial strategies and associated billing structures to remain flexible and responsive during the changing dental landscape. MDI is not an overnight change, and it has alternative payment models associated with quality improvement programs that are constantly being evaluated and refined.
Consistent networks are also important for member benefit design; this is how you ensure continuity of care and establish interprofessional care teams that support oral health case management and care coordination efforts. It becomes imperative that the networks across different eligibility criteria (e.g., Medicaid and Medicare) are not only the same but also integrated across physical, behavioral, oral health, and more.
Next steps: Profound oral health disparities have only become more pronounced since the COVID-19 pandemic. Given that health outcomes improve and health costs decrease when patients receive dental care, MDI just makes sense, especially in the dual space where outcomes are worse and health costs soar.
To get there, everyone involved in dental care delivery, including software vendors, payers, policymakers, and dental providers, has a role. We need comprehensive dental benefits, and they should be standard offerings for any person. We need to address the disconnect between public insurance programs where dental benefits may overlap. We need a better patient experience; health plans and dental benefit administrators must partner to create a holistic MDI experience for members that will make progress in all four components of the quadruple aim.
Now is the time to step up and take advantage of the transformational momentum sparked by pandemic-related care delivery changes.
Editor's note: This article appeared in the December 2022 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
References
- Oral health. World Health Organization. March 15, 2022. https://www.who.int/news-room/fact-sheets/detail/oral-health
- Freed M, Neuman T, Jacobson G. Drilling down on dental coverage and costs for Medicare beneficiaries. KFF. March 13, 2019. https://www.kff.org/report-section/drilling-down-on-dental-coverage-and-costs-for-medicare-beneficiaries-issue-brief/
- Katch H, Van de Water PN. Medicaid and Medicare enrollees need dental, vision, and hearing benefits. Center on Budget and Policy Priorities. December 8, 2020. https://www.cbpp.org/research/health/medicaid-and-medicare-enrollees-need-dental-vision-and-hearing-benefits
- Wadhera RK, Wang Y, Figueroa JF, et al. Mortality and hospitalizations for dually enrolled and nondually enrolled Medicare beneficiaries aged 65 years or older, 2004 to 2017. J Amer Med Assoc. 2020;323(10):961-969. doi:10.1001/jama.2020.1021
- Elmaleh-Sachs A, Schneider EC. Strange bedfellows: Coordinating Medicare and Medicaid to achieve cost-effective care for patients with the greatest health needs. J Gen Intern Med. 2020;35(12):3671-3674. doi:10.1007/s11606-020-05914-y
- Johnston KJ, Mittler J, Hockenberry JM. Patient social risk factors and continuity of care for Medicare beneficiaries. Health Serv Res. 2020;55(3):445-456. doi:10.1111/1475-6773.13272.
- People dually eligible for Medicare and Medicaid. CMS. March 2020. https://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/Downloads/MMCO_Factsheet.pdf
- Simon L. Overcoming historical separation between oral and general health care. Interprofessional collaboration for promoting health equity. AMA J Ethics. 2016;18(9):941-949. doi:10.1001/journalofethics.2016.18.9.pfor1-1690
- System transformation: A three domain framework to innovating oral health care. CareQuest. October 2020. https://www.carequest.org/system/files/CareQuest-Institute-Three-Domain-Framework-White-Paper.pdf
- Missed connections: Providers and consumers want more medical-dental integration. CareQuest. https://www.carequest.org/system/files/CareQuest_Institute_Missed-Connections-Providers-and-Consumers-Want-More-Medical-Dental-Integration_FINAL.pdf
- Return on investment. Healthcare investment savings. CDC. Page last reviewed August 25, 2020. https://www.cdc.gov/oralhealth/infographics/roi-healthcare.html
- Thakkar-Samtani R, Heaton LJ, Kelly AL, et al. Diabetes treatment costs decrease after periodontal therapy. CareQuest. https://www.carequest.org/system/files/Samtani_NOHC-2022%20poster_48x36_3.31.22.pdf
- Borah BJ, Brotman SG, Dohlakia R, et al. Association between preventive dental care and healthcare cost for enrollees with diabetes or coronary artery disease: 5-year experience. Compendium. March 2020. https://www.aegisdentalnetwork.com/cced/2022/03/association-between-preventive-dental-care-and-healthcare-cost-for-enrollees-with-diabetes-or-coronary-artery-disease-5-year-experience
- Value-base care: The federally qualified health center story. CareQuest. https://www.carequest.org/resource-library/value-based-care-federally-qualified-health-center-story
- Mosen DM, Banegas MP, Dickerson JF, et al. Examining the association of medical-dental integration with closure of medical care gaps among the elderly population. J Am Dent Assoc. 2021;152(4):302-308. doi.org/10.1016/j.adaj.2020.12.010
About the Author

Dave Olson
Dave Olson is the Senior Vice President of Business Development, Medicare Advantage and National Accounts for DentaQuest, where he focuses on delivering innovative dental solutions that serve the quadruple aim of better quality, lower costs, better member experiences, and better provider experiences. With more than 10 years experience in management consulting for the health care payor market, he leads business development, Medicare Advantage, and national accounts for DentaQuest.