No Shrink? No Stress? No Problems
By Jason Olitsky, DMD
The “bread and butter” procedures of everyday general dental practices are typically direct posterior composite restorations. Unfortunately, the traditionally technique-sensitive nature of placing these restorations (for example, open- or closed sandwich layering techniques) has left many clinicians feeling less than confident with their selected protocol, particularly when patients present with large defects requiring treatment.1
As a result, indirect restorations may be preferred to avoid complications like postoperative sensitivity, less-than-ideal aesthetics, improper contacts, or voids in the material or unfilled margin areas.2–4
Today, however, bulk-fill materials enable clinicians to easily modify their direct posterior composite placement protocol to consistently achieve ideal results. Among the characteristics of today’s bulk-fill materials that contribute to treatment predictability and ease of placement is their ability to be placed in a single increment, or with a liner, to reduce the likelihood of voids. Additionally, bulk fill composites demonstrate a deeper depth of cure (about 4 millimeters), which minimizes the chances of undercuring the material and thus reduces the possibility of postoperative sensitivity.
The following case demonstrates how efficiently direct posterior composite restorations can be placed using bulk-fill materials. The protocol optimizes the material’s handling characteristics and working time for adaptation, establishing proper contacts and sculpting lifelike anatomy.
Case report
A 62-year-old male patient presented with defective amalgam restorations on the distal/occlusal surfaces of tooth #13 and the mesial/occlusal/lingual surfaces of tooth #14, which also had a separate buccal amalgam restoration (Figs. 1 and 2).

Although crowns or onlays would typically be the preferred treatment plan for such cases, the patient indicated the need to postpone such restorations for a couple of years. Because of the depth of the existing restorations and the recurrent caries present, it was wisest to initiate caries control and restoration of the teeth.
When treating posterior cavities of this size, the choice of composite material can make clinical procedures much more efficient and predictable while producing a high level of aesthetics. My choices are bulk-fill materials such as Tetric EvoFlow Bulk Fill or Tetric EvoCeram Bulk Fill, both from Ivoclar Vivadent.
The patient was anesthetized and a nonlatex Hygenic brand dental dam was placed with a NW clamp on the second molar (Fig. 3). Using a Brasseler 6845KR.31.018 diamond, the defective amalgam restorations were completely removed, after which the deeper portions of the box were beveled
using a Brasseler 6856 018 diamond. The cavosurface margins were then beveled to increase the enamel bonding area and enhance aesthetics (Fig. 4).
The completed preparations were particle-abraded using a PrepStart air abrasion unit from Danville with a 90-degree, .015 tip and 27-micron aluminum oxide powder. This step homogenized the dentin and sealed the dental tubules, and would help to increase the bond to dentin and reduce sensitivity.
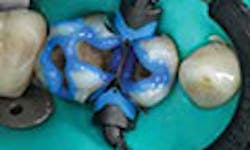
To facilitate sealing the preparation and forming the adaptive layer for the composite restorations, a Compsit-Tight 3D ring with a slick band and Composi-Tight 3D Fusion wedge, both by Garrison, were placed (Fig. 5). It is important during this step to ensure a tight interface between the band and tooth to enable ideal adaptation of the direct restoration to the margins.

Selective etching protocol followed, using Ultra-Etch 35 percent phosphoric acid for 15 seconds on the enamel only (Fig. 6), after which the preparations were thoroughly rinsed. One coat of Adhese Universal bonding agent was applied to the selectively etched preparations using a VivaPen (Fig. 7), dried with ADEC oil- and moisture-free air (Fig. 8), and light-cured with a pair of Bluephase Style LED curing lights for 10 seconds per tooth (Fig. 9).
Unlike the traditional flowable materials that must be placed as a thin increment to minimize shrinkage stresses and ensure complete curing, Tetric EvoFlow Bulk Fill Shade (IVA) was used for the first increment. It can be placed in increments up to 4mm without concerns about shrinkage stresses or incomplete curing, and its self-adapting technology contributes to void-free restorations in the deepest boxes. Aesthetically, dark underlying tooth structure is blocked by the similar dentinlike opacity that’s achieved after a 10-second cure per tooth (Fig. 10).
A single, final increment of Tetric EvoCeram Bulk Fill in Shade IVA was placed from a compule by injecting directly into the preparation. The composite was gently condensed with a multiuse composite
instrument and shaped with a Cosmedent 8A composite instrument (Fig. 11). This increment was cured for 10 seconds using Bluephase Style LED curing lights from the occlusal surface.

After the bands were removed (Fig. 12), the restorations were cured for an additional 10 seconds from the proximal surfaces to ensure complete curing (Fig. 13). The composite was contoured with a Brasseler 8274.31.016 flame, and the occlusion was checked and adjusted. Margins were defined
with Cosmedents medium-grit Flexi Disk, after which the restorations were polished with Astropol polishing points (Figs. 14–16).
Conclusion
I’ve found that placing everyday direct posterior restorations is easier, less time-consuming, and less technique-sensitive when materials like Tetric EvoFlow Bulk Fill and Tetric EvoCeram Bulk Fill are used according to the technique described (Fig. 17 and 18). The properties of these materials reduce shrinkage stress, minimize postoperative sensitivity and help to prevent marginal failure—all of which translates to more predictable posterior direct composite restorations, even for large defects.
References
1. Wieczkowski G Jr, Joynt RB, Klockowski R, Davis EL. Effects of incremental versus bulk fill technique on resistance to cuspal fracture of teeth restored with posterior composites. J
Prosthet Dent.1988;60(3):283-287.
2. Van Ende A, De Munck J, Van Landuyt KL, et al. Bulk-filling of high C-factor posterior cavities: effect on adhesion to cavity-bottom dentin. Dent Mater. 2013 ;29(3):269-277. 54
3. Kwon Y, Ferracane J, Lee IB. Effect of layering methods, composite type, and flowable liner on the polymerization shrinkage stress of light cured composites. Dent Mater. 2012;28(7):801-809.
4. Olmez A, Oztas N, Bodur H. The effect of flowable resin composite on microleakage and internal voids in class II composite restorations. Oper Dent. 2004;29(6):713-719.
About the author: Jason Olitsky, DMD, maintains a private practice in Ponte Vedra Beach, Florida. Olitsky is past president of the Florida Academy of Cosmetic Dentistry, an accredited member of the American Academy of Cosmetic Dentistry and an accredited Digital Smile Design master. As director of aesthetics and photography with Clinical Mastery Series, he teaches portrait and clinical photography and over-the-shoulder anterior aesthetics courses. Olitsky also is clinical adjunct faculty with the Arizona School of Dentistry and Oral Health and a clinical consultant for Dental Advisor, and co-wrote The Naked Tooth: What Cosmetic Dentists Don’t Want You to Know, a book aimed at a general consumer readership.
Originally published in the April, 2017 issue of Dentaltown magazine. Reprinted with permission from Dentaltown magazine.