Fixed vs. removable implant-supported prostheses
Key Highlights
- Both fixed and removable implant-supported prostheses offer distinct advantages, and patient preferences often vary based on comfort, hygiene, cost, and esthetics.
- Fixed options provide stability and a natural feel, while removable prostheses offer easier maintenance, lower cost, and simpler repairs.
- Dentists should prioritize patient education and shared decision-making to determine the most appropriate treatment for each individual case.

Each month, Dr. Gordon Christensen answers a question from readers about everyday dentistry.
Q: The dental journals and magazine articles are replete with how to treat edentulous patients with a fixed prosthesis. I have treated many edentulous patients with both fixed and removable prostheses, and I have found that many of my patients prefer implant--supported removable prostheses instead of fixed prostheses. Why is so much emphasis being placed on fixed prostheses? In my experience, patients should be provided with education about both alternatives and allowed to decide which is best for their specific situation. Am I wrong in this assumption?
A: Your question is very important! The opinions of edentulous patients about having no teeth varies significantly. Most tolerate their typical maxillary denture well and appreciate not worrying about dental caries or periodontal disease. It has been my observation that most dislike their mandibular denture and find it to have inadequate retention, continuing sore spots, and instability during chewing.
Additional reading: Which is best: A 3-unit fixed prosthesis or an implant and crown?
Some feel guilty and embarrassed about having missing teeth and try to hide their edentulism, while others consider their condition to be related to their stage in life and take it with toleration.
When root-form titanium implants became available for the profession about 40 years ago, a significant paradigm change occurred. Fixed dentures could be placed on osseointegrated implants.
The original Brånemark design used six implants in the maxillary arch placed anterior to the maxillary sinus parallel to one another. Six implants were also placed in the mandibular arch anterior to the mental foramen and parallel to one another. A cantilever supported by the six implants on each arch was placed distal to the implants.
During the initial introduction of this concept, I placed numerous fixed prostheses for edentulous patients. Techniques were developed to have the screwed--on prostheses contoured to allow patients to clean under them with toothbrushes, floss, pipe cleaners, water lavage devices, or whatever could be used to reach under the pontics.
My seating procedure for the prostheses was as follows:
Initial seating appointment: Additional contouring of pontics to allow optimum cleaning under them, placing the screws into the implants, refining the occlusion, placing only cotton in the screw access holes, and educating the patient on how to clean the prosthesis, implants, and gingival tissue
Secondary seating appointment 24 hours or more later: Remove the prosthesis, determine areas irritating soft tissue and collecting food, adjust those areas, adjust occlusion, replace the prosthesis and screws, refine occlusion, placing only cotton in the screw access holes, or fill the holes using your normal composite procedure.
Potential third adjustment appointment one week later: Occasionally this appointment is necessary, if the patient is still unable to accomplish optimum oral hygiene. Refine the pontic areas and occlusion and fill the access holes with your normal composite procedure.
Final initial seating appointment four months later: Check occlusion and hygiene. If the patient is doing well, place them on one-year prosthesis removal, dental hygiene prophylaxis, and exam of prosthesis and implants.
The above procedure allows adjustment of the new prosthesis periodically, greatly reducing the challenges of food impaction and bad breath, potential developing implant failure, and observation and repair of any other challenges.
Currently, I do not see this type of progressive prosthesis seating procedure primarily because of early seating, nonremoval and adjusting of the prosthesis, and even one--day tooth removal and seating the prosthesis on the same day. The result is gingival irritation, bad breath, inadequate esthetics, and other maladies.
I prefer tooth removal when necessary, placement of an interim complete denture worn by the patient for a few months to allow optimum bone healing, followed by implant placement and prosthesis seating.
At that time, the bone has matured and optimum implant placement and prosthesis development can be done. Subsequently, I suggest a modification of the above seating technique specifically for each patient.
I have just described my optimum concept. Many modifications of it can and should be accomplished for specific patients.
Advantages of fixed implant--supported prostheses for edentulous patients (figure 1)
- The prosthesis does not have to be removed.
- The patient has the feeling of natural teeth.
- The prosthesis is solidly in place and does not move.
- The above advantages provide a positive psychologic feeling for the patient.
When properly designed and fabricated, fixed prostheses for edentulous patients can be effective both from physiologic and esthetic standpoints, and they are greatly appreciated by patients. However, frequently, the prostheses could be better designed.
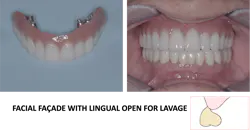
Advantages of removable implant--supported prostheses for edentulous patients (figure 2)
As would be expected, patient preferences concerning either fixed or removable prostheses vary considerably. Clinicians Report Foundation (CR) has polled their clinical evaluators, project directors, and patients and found many prefer the removable option.
- Esthetics is better because properly designed flanges can be placed on the denture filling the face to its original anatomic form.
- Oral hygiene is faster and easier since the prosthesis can be removed and cleaned at will. Observation and implant cleaning is simple. Recare appointments are simple and shorter.
- Repair is easy. If an implant fails or the prosthesis needs repair, the procedures are relatively simple and usually the denture can still be used.
- The cost of the removable prosthesis is significantly lower by about one-third.
- The implants can be cleaned and maintained easily. If an implant has failed, another one can be placed in another site, and usually the denture can be repaired to accommodate the new implant.
- Usually, bone removal is not necessary.

Summary
It is the responsibility of dentists to provide education and informed consent for patients relative to the treatments possible for their edentulism. The two major alternatives related to implants are implant-supported fixed or removable prostheses. Each alternative has positive and negative characteristics as discussed in this article. Which is best for a specific patient relates directly to a mutual decision made by the dentist and patient.
Editor's note: This article appeared in the May 2026 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
About the Author

Gordon J. Christensen, DDS, PhD, MSD
Gordon J. Christensen, DDS, PhD, MSD, is founder and CEO of Practical Clinical Courses and cofounder of Clinicians Report. His wife, Rella Christensen, PhD, is the cofounder. PCC is an international dental continuing education organization founded in 1981. Dr. Christensen is a practicing prosthodontist in Provo, Utah.