Can recurrent caries be prevented by glass ionomer?
Key Highlights
- Caries is largely preventable, but patient compliance is the biggest barrier, making noncompliance-dependent strategies especially valuable in high-risk patients.
- Glass ionomer remains the only restorative category with true cariostatic benefits, offering chemical bonding to tooth structure, fluoride release, and better sealing than composites.
- Modern glass ionomers have improved handling and strength, making them a strong option for crown cementation and restorations in caries-active pediatric, teen, and senior patients—despite ongoing esthetic and wear limitations.

Each month, Dr. Gordon Christensen answers a question from readers about everyday dentistry.
Q: One of my major practice frustrations is my inability to keep patients caries free. Despite having excellent hygienists who educate our patients well and trying my best to make my restorations as well done as possible, I still see caries continue to recur in many patients. Does dentistry have the materials, technologies, preventive concepts, and the dentist’s clinical abilities to predictably stop caries?
A: You have stimulated me to respond with a few research-based insights. Your question has a few challenges that make it difficult to definitively answer.
Dental caries is a preventable disease for most people. Dentistry and dental research have shown many ways to prevent caries, but most patients don’t use the preventive diet and oral hygiene concepts that reduce or eliminate caries development. They eat cariogenic foods and drink caries-producing beverages and leave the debris in their mouths. That is the major reason dental caries is the most frequent childhood disease, and for most people the disease continues throughout life, eventually causing loss of some or all their teeth. Changing our patients’ diet and oral hygiene habits is nearly impossible to prevent caries without using some concept that doesn’t rely on patient compliance for success (figure 1).
Please visit Clinicians Report Foundation if you are seeking resources for the information below (cliniciansreportfoundation.org).
Some dental restorative materials have been proven to prevent dental caries. Dentists can and should place cariostatic restorative materials for some or all patients to reduce or eliminate caries. The degree of cariostatic effectiveness among dental products varies markedly, but one category—glass ionomer—is well known to highly resist caries development. This material was introduced into dentistry in 1972. It consists of an acid-base reaction between a fluoroaluminosilicate glass powder, and an aqueous solution of polyacrylic acid (PAA). Unlike other materials of that time, it provided chemical adhesion (chelation) to enamel and dentin, fluoride release, and thermal expansion like tooth structure. It was well received in some geographic areas and shunned in others, including the US.
Why was glass ionomer not accepted well in some geographic areas?
During the setting period, the material was sticky, hard to control in its initial, slightly putty stage, and slow to set. Additionally, it had low strength compared to composite resins, dissolved in some acids, and was opaque, making it almost impossible to match color with teeth.
On the positive side, it chelated to tooth structure, released significant fluoride ion during its dissolution, had no open margins with tooth structure, and established a reputation of being the only dental restorative material with these positive characteristics. As of 2025, it is still the only category of dental materials with these highly desirable properties.
Has glass ionomer been improved in recent years?
Yes, glass ionomer has been improved and is continually being improved. Some of the improvements based on numerous studies and reported practitioner empirical evidence are:
- Significantly improved working characteristics, including less stickiness, better working time, and improved consistency
- Higher viscosity with capsule-based delivery
- Bioactive glasses and/or hydroxyapatite have been added for potential remineralization of adjacent tooth structure, both dentin and enamel.
- Faster set and higher early strength caused by modifications, including resin inclusion, resin-modified glass ionomer (RMGI), and improved powder-liquid ratios. These changes allow earlier finishing.
- Better esthetics caused by smaller filler particles (nanofillers), resulting in improved translucency, and somewhat better polish potential
- Examples of improved glass ionomer brands are Equia Forte from GC, Ketac Universal from Solventum (3M), and others.
Are there still limitations for the improved glass ionomers?
Yes, the more significant limitations of glass ionomers are:
- Faster wear than composite, compromising clinical longevity
- Lower strength than composites
- Esthetic result is inferior to composite.
- Slow set makes finishing slower than composite.
- Handling properties not as acceptable as composite
- Can require longer to place than composite
- When resin is added (resin-modified glass ionomer), chelation is reduced and margin opening is increased.
When and how should the improved glass ionomers be used?
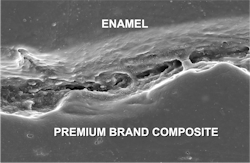
Current composites are not cariostatic and have microscopically open margins. They do not seal tooth preparations (figure 2).
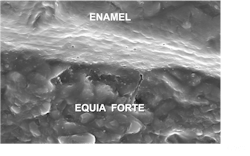
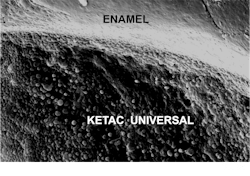
Glass ionomers seal tooth preparations and are cariostatic (figures 3 and 4). But glass ionomers still have some limitations listed above.
Best locations and techniques for glass ionomers:
- Glass ionomer (GI) or RMGI cement is a first choice for crown cementation.
- GI or RMGI restorations for caries-active senior adults with continuing dental caries (figures 5 and 6)
- GI or RMGI restorations for teenagers with ongoing poor oral hygiene and continuing caries activity
- GI or RMGI restorations for pediatric patients with high caries potential or significant caries activity
- GI or RMGI liners, bases, or a major portion of the restoration used under a composite external layer
- GI used as the apical one-third or more of box forms in caries-active patients


Summary
Glass ionomers have been used for over 50 years with only moderate acceptance because of numerous clinical challenges. However, they are the only dental restorative material that bonds chemically to tooth structure and has significant cariostatic properties. Fortunately, several changes in glass ionomers have been made in recent years, making them more clinically acceptable. As a result, their use should now be frequently considered because of these improvements. This article identifies the strengths and limitations of glass ionomers and makes suggestions for the uses of the new glass ionomers.
Editor's note: This article appeared in the March 2026 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
About the Author

Gordon J. Christensen, DDS, PhD, MSD
Gordon J. Christensen, DDS, PhD, MSD, is founder and CEO of Practical Clinical Courses and cofounder of Clinicians Report. His wife, Rella Christensen, PhD, is the cofounder. PCC is an international dental continuing education organization founded in 1981. Dr. Christensen is a practicing prosthodontist in Provo, Utah.