What are the best procedures for composite tooth preparations?
Key Highlights
- Proven step-by-step procedures for composite tooth preparations across all G. V. Black classifications
- How to achieve effective tooth disinfection and desensitization using glutaraldehyde-based solutions
- Clinical guidelines for managing deep caries and pulp exposures with indirect and direct pulp capping techniques

Each month, Dr. Gordon Christensen answers a question from readers about everyday dentistry.
Q: I have listened to many CE courses on composites and have placed hundreds of restorations, but I hear about various differing sequences and techniques promoted for preps of different depths. What is the preferred procedure for composite tooth preparations to provide both tooth disinfection and desensitization, and is it the same for various G. V. Black classes of need and depth of caries?
A: There are many different techniques for the most appropriate sequence of steps and materials for typical resin-based composite tooth preparations. Most of the techniques are similar and can work adequately for all G. V. Black classifications. Clinicians Report Foundation (CR) has studied this procedure and the necessary materials for nearly 50 years. The following information lists the clinical steps, proven example materials, and the rationale for each in chronological order. The following successful procedures have been researched repeatedly, and videos on their use are listed later in this article. Many other material brands and procedures can be used. The example products described represent only some of the proven products.
No. 1: Anesthetic
Articaine 4% with 1:100,000 epinephrine is the most-used local anesthetic in dentistry. Assuming there are not any known patient challenges with vasoconstrictors or articaine, this anesthetic is highly effective.
Articaine is more effective than lidocaine. Using only one-half cartridge delivered as an infiltration through a 30-gauge needle is usually adequate.
However, if the patient has had previous challenges becoming anesthetized, some dentists prefer blocks over infiltrations.
Buffering local anesthetic with sodium bicarbonate is becoming more popular in dentistry and has been used in other parts of medicine for years. Buffering has been proven and allows treatment without pain almost immediately after injection.
Two brands are popular: Onset by Onpharma and Buffer Pro from Septodont.
When using a buffered anesthetic, waiting about one minute before starting treatment is usually adequate.
No. 2: Tooth preparation
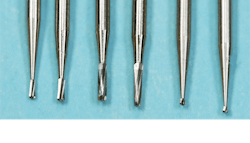
The following procedures are suggested for all classifications of resin-based composite use. The most popular burs for typical initial class I and class II restorations are #330 for the isthmus width of a molar and #329 for the isthmus width of a premolar or diamond rotary instruments of similar size and shape (figures 1 and 2).

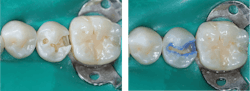
Normal depth tooth preparation. After making the tooth preparation, etch it using your preferred procedure (total etch, selective etch, or self-etch). I prefer selective enamel etch of enamel only, but any of the three ways works. Etch 15 seconds in a nonfluoride area, or 20 seconds in a geographic area with community water fluoridation (figures 3 and 4).

Wash and gently dry the prep.
Place two one-minute applications of glutaraldehyde-containing liquid or gel on the entire prep. Popular products are Gluma from Kulzer or MicroPrime G from Zest Dental Solutions. There are several similar products available, and all contain 5% glutaraldehyde and 35% hydroxyethyl methacrylate (HEMA). As proven by CR research, two applications are necessary for the medication to reach the pulp and disinfect the tooth prep.
This well-proven technique disinfects and desensitizes the prep. Proper use provides an excellent result with profound disinfection of the dentinal tubules and desensitization of the tooth.
Suction the solution off to avoid gingival tissue irritation. Do not blow air on it. Do not wash the solution off. Doing so reduces the medication effect.
Continue with placing bonding agent and restorative resin of your choice. The brands of bonding agents and restorative resins have become very similar since composite resin has been in use since the late 1950s. According to CR surveys, the Solventum (3M) products are most popular (Scotchbond Universal Plus and Filtek Supreme Ultra). Other widely used brands are Kerr, Ivoclar, GC, Dentsply Sirona, and many others.
Deep tooth preparation, no pulp exposure. An indirect pulp cap is indicated. Prepare the peripheral areas of the prep first, leaving the deep caries for later to avoid pulpal contamination if a pulp exposure occurs. After removing the deep caries and not having a pulp exposure, acid etch the entire prep, place glutaraldehyde as above followed by a 1 mm thick insulating bioactive liner on the deepest areas. Proven bioactive products are MTA Flow from Ultradent, Vitrebond Plus from Solventum (3M), Fuji Lining Cement from GC America, and others.
Pulp exposure. A direct pulp cap may be indicated. Carefully accomplish the previous preparation procedure for deep preps, avoiding a pulp exposure if possible. If an exposure occurs and is 1 mm or less in diameter with normal appearing blood slowly coming from it, the following direct pulp cap technique has been shown to be effective and usually successful:
Etch the enamel margins for 15 seconds and wash off the acid.
Stop the minor bleeding coming from the pulp exposure by placing styptic material on a cotton pellet on the bleeding site for about three seconds. Astringedent from Ultradent (ferric sulfate and ferric subsulfate) or Viscostat Clear from Ultradent (aluminum chloride) have been used for years for this purpose.
If the bleeding has not stopped in three seconds, try another three seconds. If that still does not stop the bleeding, consider doing endodontic treatment because the pulp may be hyperemic.
Accomplish the glutaraldehyde two-minute procedure on the entire prep, including the minor exposure. Glutaraldehyde is a fixation solution and has clinical empirical evidence for success, but more long-term research is underway for further validation.
Place the same bioactive-insulating products described above for an indirect pulp cap.
Air thin it, and cure.
No. 3: Place and finish the restorative composite as usual
A future article will follow on the best methods to place and finish the composite to produce a nonsensitive, long-lasting restorative service.
Summary
Currently, almost all direct dental restorations are resin-based composite. Although resin restorations are not serving as long as amalgam, composite resin restorations can be beautiful and relatively long-lasting when placed properly in small preparations. Some dentists report that their composite restorations still have postoperative tooth sensitivity. This article explains how to eliminate that challenge, and how to accomplish indirect and direct pulp caps if needed.
Editor's note: The article appeared in the November/December 2025 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
About the Author

Gordon J. Christensen, DDS, PhD, MSD
Gordon J. Christensen, DDS, PhD, MSD, is founder and CEO of Practical Clinical Courses and cofounder of Clinicians Report. His wife, Rella Christensen, PhD, is the cofounder. PCC is an international dental continuing education organization founded in 1981. Dr. Christensen is a practicing prosthodontist in Provo, Utah.