In-office 3D printing is growing. Is it right for your practice?
Key Highlights
-
3D printing in dentistry is rapidly expanding, offering efficient, cost-effective solutions for producing study models, splints, surgical guides, and temporary restorations—though it remains in the early adoption stage for permanent crowns and prostheses.
-
Successful implementation depends on your practice setup and preferences, including willingness to learn or delegate lab-style procedures, available space, and staff training.
-
Initial costs are increasingly manageable, with entry-level systems starting around $5,000, and many dentists reporting that savings in lab fees and turnaround times can offset the investment.

Each month, Dr. Gordon Christensen answers a question from readers about everyday dentistry.
Q: I am a young practitioner asking for your help. After a couple of years of private practice, I am frustrated with my lack of knowledge about many of the technologies I see advertised. I was introduced to only a few of them in dental school. All the ads I see promote their technology like it is better than analog, yet they are usually far more expensive than their analog competitors. I am confused! The technology I am considering is in-office 3D printing. Is it worth buying and learning how to use?
A: 3D printing is not a new concept. It has been around a long time in the lay world. It is just new to dentistry. Whether you should get it for your practice depends on several of your personal and practice characteristics. Some of them are:
- Do you enjoy doing some dental laboratory procedures? Many dentists do not prefer to do laboratory work and instead delegate all of it to laboratory technicians, while others enjoy it. Consider the history of the in-office milling procedure. Although in-office milling devices are well proven and can provide an excellent clinical result if accomplished properly, most dentists prefer to have a laboratory make their crowns and fixed prostheses. Most dentists using 3D printing delegate the procedure to qualified, educated staff members. However, some dentists enjoy the creativity of making printed objects for their patients.
- Do you delegate some clinical procedures to your staff, and do you have an adequate number of staff to whom you could delegate another procedure? In Clinicians Report Foundation (CR) surveys, we have found that most dentists educate a staff member to accomplish this clinical task. Is it a difficult task? That depends on the object you are printing.
- Do you have benchtop space in your lab area to place the printing devices? The typical 3D printing device (figure 1) can be set up on a table or benchtop area in a few feet of space. Some dentists place a vent over their printing device to remove any offensive odors that may occur.
The 3D printing procedure may appear to be more difficult than you would like. Only you can determine if you want to learn this procedure or if you want a lab to accomplish it for you.
If you are considering in-office printing, are you planning to do the printing yourself or delegate the printing procedure to your staff? Those dentists currently using 3D printing report to me in large CE courses that there is a learning curve that takes a while, but most say the procedure is relatively simple after doing it for a short time.
What tasks are added when incorporating the 3D printing procedure?
Processing: 3D printing requires a digital impression made by a typical intraoral scanner, the most popular of which are iTero, CEREC, and 3-Shape. Then comes making a 3D file, usually in STL using dental CAD software to edit the file, creating a base for the model, slicing the model, selecting the material, exporting the file, loading the resin cartridge or vat with the resin, transferring the sliced file to the printer, and starting the print, which requires from 30 minutes to several hours to print.
Postprocessing: includes washing and curing
Finishing: includes smoothing and polishing
Storage: There are many reasons for storage of the used 3D models or data, such as potential legal challenges, patient education, etc.
Simplified summary of the above steps:
- Scan
- Clean the scan
- Edit
- Slice
- Wash
- Cure
- Finish
- Use the print and store the data for future use
What procedures are most frequently printed in dentistry?
Recent surveys conducted and published by Lab Management and Clinicians Report Foundation respectively are available and show that most dentists are printing primarily intermediate longevity need objects, such as those listed below. Which of these popular 3D printing procedures would be appropriate for your practice?
- Study models for specific patient cases
- Educational models for patients
- Occlusal splints
- Surgical guides
- Temporary or intermediate crowns or prostheses
- Models for clear aligners
- Custom impression trays
Why do these surveys not show crowns and fixed prostheses as popular 3D procedures?
Currently, ads in magazines and articles promote printed resin crowns and fixed prostheses. In my opinion, every technology goes through the same cycle before it is accepted or rejected. At the time of this article, 3D printing is what I call in the early adaptor stage. Only a few course attendees in the large groups to which I speak are currently printing in-office. Most are very optimistic about it for the intermediate longevity need procedures, but almost none are currently printing crowns or fixed prostheses. In-office printing must be used for several years to prove itself as financially acceptable and practical.
Some of the resins we have evaluated to date are not strong enough nor have enough filler content to be considered for long-term service. Others, such as Rodin resin from Pac-Dent, have higher filler content and are promising in CR research (figures 2 and 3).


What are potential uses for resin crowns?
It is well known that the most-used crowns currently are zirconia of various iterations. Zirconia ceramic crowns are serving well if the strongest zirconia (3Y full strength) is used for situations of high occlusal load, the anatomy from an anatomy library has been selected correctly by the lab tech, the margins are as adequate as can be expected from the milling machines, the occlusion is acceptable, and a cariostatic cement such as RMGI (RelyX Luting or Fuji Cem Evolve), or conventional GI (Fuji I or Ketac Cem) is used. Why do we need another type of esthetic crown?
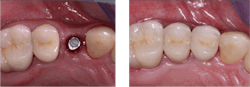
Implants do not move in bone. Teeth move significantly. When an implant is placed in a mouth of moving teeth, it should have a crown on it that wears somewhat to accommodate that phenomenon. A fully filled, strong resin crown would satisfy that need, and it is needed immediately (figure 4)! There are several other potential long-term uses that could be identified.
Setting up for printing does not have to be an expensive technology. Entry-level dental printing setups are in the range of $5,000–$7,500. Midlevel setups can range from $7,500–$15,000, and high-end can be from $15,000–$50,000. Although this may sound high, the cost and time savings soon pay for the initial investment.
After considering the advantages and limitations of this technology, does it appear to satisfy your clinical and revenue needs?
Summary
In-office 3D printing may not be for everybody. However, this newly introduced technology is growing rapidly and providing in-office, efficient, relatively fast, cost--effective, intermediate-term products with some developing promising long-term uses for printed resin crowns.
Editor's note: This article appeared in the October 2025 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
About the Author

Gordon J. Christensen, DDS, PhD, MSD
Gordon J. Christensen, DDS, PhD, MSD, is founder and CEO of Practical Clinical Courses and cofounder of Clinicians Report. His wife, Rella Christensen, PhD, is the cofounder. PCC is an international dental continuing education organization founded in 1981. Dr. Christensen is a practicing prosthodontist in Provo, Utah.