Biomimetic/bioactive direct placement tooth restoration of premolars having preeruptive subenamel caries
Croll and Cavanaugh described tissue-specific stratification of restorative materials in 2002.1 In that work, dentin was replaced with a resin-modified glass-ionomer (RMGI) cement (Vitrebond, 3M Oral Care), which chemically bonds to dentin without acid-etching or a bonding agent, albeit with a low bond strength.2 A resin-based composite material was used as the enamel replacement to complete the restoration.
Glass ionomer cements, including RMGIs, are well tolerated by the underlying pulp, have a leachable fluoride component, and expand and contract with tooth temperature changes, which contributes to maintaining the intimacy of the bond.2 The overlying composite bonds to the resin component of the photopolymerized RMGI and provides strength, wear resistance, and esthetics. The periphery of the cavosurface margin is acid-etched, and a bonding agent is applied before placing the composite.
Replacing dentin with a biocompatible RMGI material and enamel with a resin-based composite is still an excellent method for the direct restoration of a tooth. However, there are now other alternatives with more recently developed materials. Dentin replacement can be achieved with cavity liners and bases—for example, TheraCal LC and TheraBase (Bisco), NeoLiner LC (NuSmile), Lime-Lite Enhanced (Pulpdent), or others. Load-bearing surfaces can now be replaced with bioactive resin-based composite materials such as Activa BioActive Restorative (Pulpdent).
This article documents the step-by-step restoration of a mandibular second premolar, which, before eruption, was diagnosed radiographically with a coronal dentin radiolucency.
The radiographs in Figures 1a, 1b, and 1c show the tooth and the adjacent first premolar with preeruption radiolucencies indicative of carious lesions. However, no clinical evidence of occlusal caries was noted when they erupted.
The authors were perplexed by this initial observation, which led to an extensive review of the literature regarding preeruptive intracoronal radiolucencies. Such intracoronal defects proved to be rare but not unusual.3-8
Seow et al. studied the prevalence of these defects on 9,919 radiographs from children aged 7.8 +/- 1.79 years.4,5 Six percent of the subjects had radiolucencies in the crowns of preeruptive permanent teeth. Of the 9,919 teeth viewed, 163 (2%) were affected. Of the 126 subjects with dentin radiolucencies, 93 had one affected tooth, 31 had two affected teeth, and two had three affected teeth. The investigators reported tooth prevalence from highest to lowest: mandibular first molar (4%), followed by the mandibular first premolar (2%), mandibular second molar (1%), mandibular second premolar (1%), maxillary first molar (1%), maxillary first premolar (1%), and maxillary second premolar (0.2%).
These quoted references were significant for reporting differences in prevalence, lack of etiological diagnosis, posteruption follow-up observation, and suggesting the most desirable clinical treatment. The literature, however, is inconclusive regarding the cause of these preeruption abnormalities.
This case report describes adjacent premolars having preeruptive subenamel occlusal caries lesions. Initial radiographic detection, diagnosis, posteruption clinical examination, and treatment are presented, along with follow-up visits over a 27-month period. In addition, detailed step-by-step photographic documentation of the restoration of the second premolar is shown.
Case study: Observation and treatment
Anomalies of the mandibular left premolars in a 7-year-old boy were first observed preeruption and later treated.
A May 14, 2019, radiographic view of the patient’s unerupted first premolar showed a radiolucent defect in the mesial coronal aspect of the tooth, ostensibly subenamel (figure 1a). A buccal or lingual coronal defect could not be ruled out at that time. No such radiolucency was evident on the adjacent second premolar.
A follow-up radiograph taken on November 29, 2022, shows the primary second molar still in place; the underlying second premolar in its developmental cystic sac can be seen. It had developed a coronal radiolucency similar to that of the first premolar (figure 1b). The primary second molar was removed at that visit.
When the first premolar erupted, it showed no evidence of an occlusal caries lesion. However, subenamel caries was revealed when the tooth was prepared for exploration followed by restoration. Two bioactive materials—Lime-Lite Enhanced base/liner and ACTIVA BioActive Restorative material—were used. Months later, the second premolar had erupted sufficiently so that it could be restored using the same procedure as the first premolar repair.

Restorative method (figures 2–5)
- Local infiltration anesthesia was achieved using articaine 4% with 200,000 ppm epinephrine.
- Using the split-dam technique, a nitrile dam was placed from the permanent first molar and stretched over the mesial surface of the canine tooth.
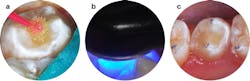
- There was no clinical evidence of the caries lesion from the occlusal aspect (figure 2a).
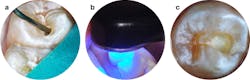
- Access to the lesion was gained with a water-cooled high-speed diamond cylinder bur.
- The carious tooth structure was debrided using slow-speed round burs (figure 2b), and cavity outline was completed with a slow-speed diamond cylinder and inverted cone carbide burs.
- The tooth preparation was disinfected with two one-minute soaks of MicroPrime G (Zest Dental Solutions; figure 2c).9,10
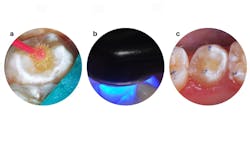
- After lightly air-drying but not desiccating the tooth, Lime-Lite Enhanced base/liner was injected with care to avoid air inclusion (figure 3a) and light-cured (figure 3b).
- The preparation was completed using a slow-speed inverted cone bur (figure 3c).
- The preparation and surrounding enamel were painted with a self-etching bonding agent (Adper Prompt L-Pop Self-Etch Adhesive).
- After 30 seconds, ACTIVA BioActive Restorative was injected to overfill, and a ball burnisher was used to spread the material so it overlapped the cavosurface margins (figures 4a and 4b).
- A curing light beam with an output of 1,100 mW/cm2 polymerized the material.
- Using a large, round diamond bur at slow speed, the hardened material was trimmed to contour (figure 4c), and a final “glaze” of bonding agent was painted and light-cured on the surface (figures 5a and 5b).
- The nitrile dam was removed and occlusion was confirmed with articulating paper (figure 5c).
- The premolars were photographed four months postoperatively (figure 6a), and a periapical radiograph of the second premolar was recorded at that time—August 2023 (figure 6b).



Discussion
As seen in this case, the presence of caries lesions in unerupted teeth is rare but not unique—reports on the subject have been published over the last few decades.4-8 What is different in this case is the careful observation of the affected teeth, both pre-and posteruption, leading to restorations using state-of-the-art materials.
According to the radiographs, the lesions appeared to be in dentin only (figures 1a, 1b, and 1c). Although radiolucencies were evident in the mesial aspects of the occlusal surfaces of the premolar crowns at different dates pre- and posteruption (figures 1a, 1b, and 1c), no occlusal decay, enamel pits, or fissures were observed clinically after the teeth erupted (figure 2a). The radiolucencies seen in the second premolar appeared to be getting larger between November 29, 2019, and May 30, 2023. This indicates an actively progressing caries lesion, and it is doubtful that varying alignments of the radiographs can explain such enlargement (figures 1b and 1c). It is noteworthy that before root development had commenced, no radiolucency in the deeply developing second premolar crown was seen on the May 14, 2019, radiograph (figure 1a).
The pathological etiology of a caries infection such as these is obscure. A review of the literature in our search did not offer a credible explanation. However, the noted lesions in these mandibular premolars are among the 1% and 2% of most prevalently occurring preeruptive lesions from the 126 that were identified by Seow et al. in their 9,919 subjects.4,5 It seems, therefore, that in the absence of clear etiological factors, the only available option for diagnosis is the use of timely radiographs. Clinical observations (in this case, after eruption and during tooth preparation) verified diagnosis and treatment decisions.
Stratification of Lime-Lite En-hanc-ed (dentin replacement) and ACTIVA BioActive Restorative (enamel replacement) were used for restoration of these premolars for several reasons. Both materials are bioactive, meaning they release and recharge calcium, phosphate, and fluoride ions. These materials share a moisture-friendly ionic resin, an elastomeric component that absorbs shock and resists fracture and wear, and mechanisms with remineralization potential. Lime-Lite Enhanced has a methacrylate-functionalized calcium phosphate component and ACTIVA BioActive Restorative has glass ionomer in an ionic resin matrix. These materials do not contain bisphenol A, Bis-GMA, or BPA derivatives. According to the manufacturer, ACTIVA BioActive Restorative combines a glass polyalkenoate (ionomer) material with a “resilient resin matrix that will not chip or crumble that chemically bonds to teeth, seals against microleakage, and releases calcium, phosphate, and fluoride.”11
The senior author has used this restorative material since 2015 with continuing success after restoring and documenting more than 6,300 primary and permanent teeth.12-18
Disclosures: The authors have no financial interest in any company mentioned in the article nor did they receive, or will receive, any type of remuneration for production of the work. Dr. Pameijer is a consultant for Pulpdent Corporation.


Editor's note: This article appeared in the June 2024 print edition of Dental Economics magazine. Dentists in North America are eligible for a complimentary print subscription. Sign up here.
References
- Croll TP, Cavanaugh RR. Posterior resin-based composite restorations: a second opinion. J Esthet Restor Dent. 2002;14:(5):303-312. doi:10.1111/j.1708-8240.2002.tb00526.x
- Nicholson JW, Croll TP. Glass-ionomer cements in restorative dentistry. Quintessence Int. 1997;28(11):705-714.
- Rankow H, Croll TP, Miller AS. Preeruptive idiopathic coronal resorption of permanent teeth in children. J Endod. 1986;12(1):36-39. doi:10.1016/S0099-2399(86)80280-1
- Seow WK, Wan A, McAllan LH. The prevalence of pre-eruptive dentin radiolucencies in the permanent dentition. Pediatr Dent. 1999;21(1):26-33.
- Seow WK, Lu PC, McAllan LH. Prevalence of pre-eruptive intracoronal dentin defects from panoramic radiographs. Pediatr Dent. 1999;21(6):332-339.
- Al-Batayneh OB, AlJamal GA, AlTawashi EK Pre-eruptive intracoronal dentine radiolucencies in the permanent dentition of Jordanian children. Eur Arch Paediatr Dent. 2014;15(4):229-236.
doi:10.1007/s40368-013-0104-x - Nik NN, Abul Rahman R. Pre-eruptive intracoronal dentin defects of permanent teeth. J Clin Pediatr Dent. 2003;27(4):371-375. doi:10.17796/jcpd.27.4.w26q821135440504
- DeSchepper EJ, Haynes JI, Sabates CR. Preeruptive radiolucencies of permanent teeth: report of a case and literature review. Quintessence Int. 1988;19(2):157-160.
- Disinfection of tooth preparations—why and how? Clinicians Report. 2009;2(11):1-2.
- Christensen R. Dental caries 2018: new insights. Dentistry Today. 2018;37(11):122-128.
- White paper. ACTIVA BioActive: a closer look at BioActive materials changes everything you know about composites, glass ionomers, and RMGIs. 5th ed. Pulpdent Corporation. 2019. https://www.pulpdent.com/activa-white-paper/
- Croll TP, Berg JH, Donly KJ. Dental repair material: a resin-modified glass-ionomer bioactive ionic resin-based composite. Compend Contin Educ Dent. 2015;36(1):60-65.
- Garcia-Godoy F, Morrow BR. Wear resistance of new Activa compared to other restorative materials [abstract]. J Dent Res. 2015;94(Spec issue A). Abstract 3522.
- Bansal R, Burgess J, Lawson NC. Wear of an enhanced resin-modified glass-ionomer restorative material. Am J Dent. 2016;29(3):171-174.
- Croll TP, Cavanaugh RR. Occlusal augmentation of an ankylosed primary second molar with no premolar successor. Inside Dentistry. 2016;12(5):80-82.
- Croll TP, Lawson NC, ACTIVA BioActive Restorative Material in children and teens. Inside Dentistry. White paper insert. 2018;14(2).
- Croll TP, Lawson NC. Tooth repair using a bioactive restorative. Dentistry Today. 2020;39(1):86-89.
- Killian CM, Croll TP. Class I glass-ionomer restoration resurfacing: a pictorial essay. Dentistry Today. 2021;40(9):84-85.
About the Author

Theodore P. Croll, DDS
Theodore P. Croll, DDS, is a diplomate of the American Board of Pediatric Dentistry. He is a 1973 Temple University School of Dentistry graduate. After serving in the US Army Dental Corps in Germany, he completed pediatric dentistry training at the University of Connecticut in 1978. Dr. Croll’s Doylestown, Pennsylvania, pediatric dentistry practice merged with Doc Bresler’s Cavity Busters in December 2018. He currently is clinical professor of pediatric dentistry at Case Western School of Dental Medicine.
Richard R. Cavanaugh, DDS
Richard R. Cavanaugh, DDS, is a retired prosthodontics specialist from Doylestown, Pennsylvania. His prior career teaching affiliations include Temple University Maurice H. Kornberg School of Dentistry and the University of Pennsylvania School of Dental Medicine.
Updated May 1, 2024
Cornelis H. Pameijer, DMD, DSc, PhD
Cornelis H. Pameijer, DMD, DSc, PhD, is professor emeritus in the department of reconstructive sciences at the University of Connecticut in Farmington, Connecticut.
Updated May 1, 2024