Ask Dr. Christensen

In this monthly feature, Dr. Gordon Christensen addresses the most frequently asked questions from Dental Economics® readers. If you would like to submit a question to Dr. Christensen, please send an e-mail to [email protected].
For more on this topic, go to www.dentaleconomics.com and search using the following key words: resin-based composites, veneers, at-home bleaching, enamel microabrasion, provisional restorations, Dr. Gordon Christensen.
Q Recently, a 23-year-old patient came to me for a second opinion about placing veneers on her anterior teeth. A local general practitioner had treatment-planned eight veneers for her upper anterior teeth, claiming that the few small diastemas, two endodontically treated, slightly discolored teeth, and superficial white spots on a few teeth required ceramic veneers to provide an adequate esthetic result. At her age, the treatment plan seemed very aggressive to me, and I tactfully suggested a more conservative plan. I’m sure I upset the other practitioner, but she decided to have me do the conservative plan, and it turned out well. Did I do the wrong thing, or would the veneers have been a more adequate long-term treatment?A I am pleased to hear that your patient was happy with the result. Placing eight veneers would have been an easier treatment plan, but it would not have served this young person well in the long term. At best, the ceramic veneers would have been adequate from an esthetic standpoint for about 10 to 20 years, at which time she would have had to have them replaced. Multiply that out over her lifetime, and the end result would have been several replacements, perhaps leading to crowns and/or endodontic treatment on some of the teeth.In my opinion, you did the right treatment, and I can predict that the patient will come back to you in the future because the conservative treatment you accomplished was obviously adequate and less expensive for her and her family. She now trusts and respects you.
I am sure some readers will disagree with my previously expressed opinion. To share some information on conservative treatment, I have elected to discuss a patient I treated conservatively about two years ago, a patient who appears to be similar to the one you described.
Figure 1 shows a 21-year-old female previously treatment-planned by another dentist for eight veneers extending from her maxillary first premolar on the left to the first premolar on the right. The image shows one slightly discolored, endodontically-treated central incisor tooth, one diastema, acceptable tooth color, and numerous superficial white spots on almost every tooth.
Placing veneers on this girl would have been relatively easy. It would have included placing a fiber-reinforced, resin-based composite post in the endodontically treated central incisor, potentially bleaching that tooth superficially.

Fig. 1 — Patient planned by previous dentist for veneers on eight teeth.
A tooth preparation appointment, a seating appointment, and an occlusal adjustment appointment would have been required after she had the veneers in her mouth for a few weeks. The fee would have been about $8,000, if we estimate the cost at current average U.S. veneer fees. This would have been a relatively simple treatment plan, and it could have been done with thin (0.3 mm veneers) or more conventionally prepared veneer (0.5-0.7 mm thick).
I did not suggest or accomplish the veneer treatment. After talking with the girl and her parents, she did not want to have veneers placed for the following reasons:
- She liked the current shape of her teeth, and placing thin veneers would have made the teeth more full (her word was “bucky”).
- Placing conventionally prepared veneers would have required removing significant tooth structure.
The family was affluent, and money was not a significant factor in the decision. Frankly, I agreed with her. What did we do for her? I will list the conservative procedures and the materials and brand names used to produce the finished result:
The minimally invasive conservative treatment included:
1. Scaling, root-planing, and polishing of all of her teeth. Her mouth was relatively clean and free of calculus, but had some staining and minor subgingival calculus.
2. Placement of a fiber-reinforced, resin-based composite post in the maxillary central incisor. The most popular brand names are Pentron FibreKor or FibreKleer. These posts have become very popular in recent years since they are easy to use, tooth-colored, relatively inexpensive, and they have been shown to compete well with metal posts for strength and service potential. The post channel was roughened with a pointed, tapered diamond instrument to increase retention of the post. The post channel was primed with the two-component, self-etch primer provided in the Ivoclar Vivadent Multilink Automix kit. The post was cemented with Ivoclar Multilink Automix resin cement. The cement was injected into the canal with a Centrix Needle Tube to reduce the number of air bubbles present in root-channel cementation, producing the result shown in Figure 2.

3. At-home bleaching was accomplished by the patient during a two-week period. Ultradent Opalescence PF 15% carbamide peroxide, containing both sodium fluoride and potassium nitrate desensitizers, was used for two 30-minute periods each day.
4. A two-week waiting period was observed to allow the color of the bleached teeth to stabilize. After at-home bleaching and a two week stabilization period, the teeth usually have at least one-half of a shade on the standard Vita shade guide return to them. You should not start restorative dentistry before that time because bonding resin will be compromised until the oxygen is released from the teeth, a few days after the bleach is completed. Also, the color for the restoration will be too light unless at least two weeks have passed since the bleach was completed. Patients should be advised that color will continue to come back into the teeth, and that “touch-up” bleaching will be necessary months and years later to maintain the bleached shade.
5. Enamel microabrasion was used to remove the “white spot” discolorations on the teeth. Two excellent products are available for this procedure. Either PREMA from Premier or Opalustre from Ultradent can be used. Both of them contain dilute hydrochloric acid (muriatic acid). This simple procedure is not done enough in the profession. Most of the procedure can be done by staff persons, and the dentist merely uses the material to remove the superficial white spots.
6. Another two-week waiting period was observed to allow the muriatic acid in the enamel microabrasion product to continue to work. Some of the white spots that still remain upon completion of the microabrasion appointment will be gone two weeks later.
7. The color of the teeth along with a shade guide tab of the selected color were recorded with a digital camera. The photos were sent to the laboratory technician after the crown prep and impression were made, which allows nearly perfect color matching. By this time, the color of the teeth is usually stable, at least for a few months.
8. A nanofill resin (Filtek Supreme Plus from 3M ESPE) was used on the same appointment as the crown preparation (No. 7) to fill the diastemas between the left central incisor and the lateral incisor.
9. The right central incisor was prepared for a full zirconia-based ceramic crown. If we had not placed the previously described post and core, the crown would have been very weak. With the post and core and build-up in place, the tooth was strengthened significantly.
10. A double-arch vinyl-polysiloxane impression was made using GC America Examix NDS material. Contrary to popular belief, double-arch trays and impressions have proved to be better from both an accuracy standpoint and their ability to reproduce occlusal guiding planes than full-arch impressions for one or two crowns.
11. A provisional restoration was made with 3M ESPE Protemp Plus bis-acryl resin.
12. The zirconia-based ceramic crown was made by the laboratory (3M ESPE Lava).
13. The crown was seated using resin-modified glass ionomer cement. The most popular brands are GC America FujiCEM and 3M ESPE RelyX Luting.
14. The occlusion was slightly adjusted a few weeks after seating the crown.
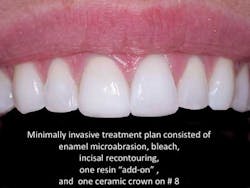
The result of the patient’s conservative treatment is shown in Figure 3. The revenue production procedures accomplished for her were:
- Adult preventive appointment
- At-home bleaching
- Enamel microabrasion
- Incisal recontouring of lower anterior teeth
- One Class IV resin-based composite
- One all-ceramic crown
The patient and her parents were pleased with the result obtained by using the conservative treatment. The procedures described here would have an average U.S. cost of approximately $1,800.
I am completely confident that providing such treatment is not only better for patients, but that it will also produce adequate revenue for practitioners in the overall perspective. You gain patient trust and confidence, and these patients send their friends and neighbors to you because of that trust.
I hope this brief discussion of conservative treatment has answered your question.
Either veneers on eight teeth or the far more conservative treatment I described would have satisfied her esthetic and functional needs. Both treatments will gradually have to be repeated in the future.
However, she can always have the more comprehensive treatment in the future if it is necessary. Eight veneers would not have been my choice if she were my 21-year-old daughter.
Two of my courses provide the techniques, materials, and devices that make restorative dentistry faster, easier, better, and more enjoyable. These courses, sponsored by Practical Clinical Courses, have continually received excellent ratings from participants for their usefulness and easily implemented information. The courses are “Rehabilitative Dentistry and Occlusion” and “Enjoyable, Profitable Fixed Prosthodontics.” For more information, visit our Web site at www.pccdental.com, or contact us by phone at (800) 223-6569.
Dr. Christensen is a practicing prosthodontist in Provo, Utah. He is the founder and director of Practical Clinical Courses, an international continuing-education organization initiated in 1981 for dental professionals. Dr. Christensen is a cofounder (with his wife, Rella) and senior consultant of CLINICIANS REPORT (formerly Clinical Research Associates), which since 1976 has conducted research in all areas of dentistry.