Don't take light curing for granted: Improper curing can lead to failure
Parag R. Kachalia, DDS
In practices around the world, resin-based restorations have become the primary direct material of choice. In addition, numerous ceramic restorations are bonded in place using light-cured adhesive and resin-based cements. There has been a drastic improvement in the physical properties of these products over the last decade; however, these improvements can only be achieved if these restorations are polymerized appropriately. Unfortunately, proper polymerization cannot be achieved simply by waving any curing light in the area of the material to be polymerized. Proper polymerization is dependent on multiple factors, including the material, the operator, and the curing light itself.
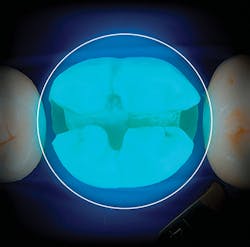
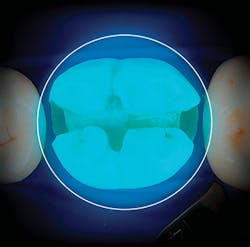
Figure 1: Visualization of the Valo Grand curing light over a 10-mm molar (107 mm2 in total)
In terms of materials, each adhesive, direct composite, and light-cured cement has a specific set of instructions in order to achieve proper polymerization. Even different shades or opacities within the same manufacturer’s composite line may require different amounts of light curing time to achieve appropriate polymerization. Historically, many researchers have shown that at the same light exposure, lighter shades with less opacity achieve a higher depth of cure compared to darker shades with greater opacity.1 Practitioners should make sure that they are aware of these curing nuances in order to provide an appropriate cure.
In addition to knowing the material properties, practitioners should also be well aware of proper curing procedures, and they should train all staff members who will be involved with curing. Curing may seem as simple as turning on the curing light. However, without proper training, numerous issues can occur. In fact, improper technique may be one of the reasons that composite restorations have a median longevity of six years.2 In a 2010 study, Richard Price and his colleagues showed a fourfold difference in energy delivered to a test specimen when the exact same light curing units were used by 20 different practitioners.3
The good news is that proper training can improve curing among dental professionals. In a study looking at dental students who had received basic light curing training, only 16% were able to deliver enough energy (6 J/cm2) to properly polymerize a restoration. After proper training using a mannequin, focusing on wearing eye protection, looking at the restoration being cured, stabilizing the light as close as possible, and paying close attention to the process, the students’ ability to properly polymerize a restoration increased to 95%.4
While this study was conducted on dental students, seasoned dental professionals may have similar results, as very few have been properly trained on curing, and surface hardness of a restoration does not equate to proper polymerization. In fact, it is not uncommon for the light to move 3–5 mm farther from the tooth once light curing is initiated due to things such as access issues, patient movement, or the operator turning to grab something for the next step of the procedure. It has been shown that the effective energy drops by 10% for every millimeter the light moves away from the surface that is to be cured.5
Assuming he or she has been well trained, the operator then needs to focus on having the right equipment and assuring that the light is operating properly. A proper light is much more than simply having high power. The minimum criteria for any curing light should be that it has the proper amount of power striking a specific surface area (i.e., irradiance), and that it emits the correct wavelength of light to cure any resin that is being used in that office.
Surface area is a critical factor, as many resins being placed today are quite large, and a curing light must have a large enough lens to adequately cure the entire surface area. It is not uncommon for a lower molar to measure 10 mm in a mesial to distal dimension, so a light must be able to effectively cure this entire surface area. If the tip of a light measures only 6 mm, an overlapping curing strategy must be employed. Simply having a larger light tip is also not enough; rather, a light should effectively cure on the periphery of the optics and not just in the middle.
In addition, access to all parts of the mouth can be challenging due to a limited range of opening or anatomical variations, so ideally a light should incorporate a low profile for proper access. As a light moves away from the tooth, a drop of energy can occur. When searching for a light, practitioners should look at units that have collimated beams to minimize the drop in energy.
In the 2014 ADA Professional Product Review, seven LED curing lights from top manufacturers were studied. Of these seven LED curing lights, only three had an effective irradiance better than the gold standard (Optilux 501, KaVo Kerr). These were the Elipar S10 (3M), the DemiUltra (KaVo Kerr), and Valo (Ultradent).6
Since the time of this review, manufacturers brought better lights to market. Most recently, Ultradent introduced the Valo Grand to improve on its original Valo cordless light that has repeatedly tested well. Similar to the original, the Valo Grand employs multiple-LED technology so that it can cure all restorative materials on the market, and it has a low profile to allow access on both adults and children. The tremendous difference, however, is that the actual size of the optics has increased by 50% to 12 mm in order to allow predictable curing of large restorations on molars (figure 1). Equally important, the light continues to be collimated across this large lens due to its refined optics, so that more predictable light curing can occur in deep box forms.
While clinical effectiveness should be the primary reason to choose a curing light, secondary considerations should include ergonomics and maintenance cost. In the Valo Grand, a second on-off button has been added to the underside of the light for better ergonomics. In addition, the light continues to maintain its robust, easily cleaned lens, and the rechargeable batteries are less than $15. Note that some replacement batteries for other LED curing lights cost over $200.
There are many areas in dentistry where one can control overhead by purchasing off-label products—but curing lights should not fall into that category. On eBay today, a dentist can find curing lights touting high power for less than $7 each. Ask yourself, are these lights anything more than a flashlight with a blue LED? Is the sensitivity a patient is having after a restoration due to poor polymerization of these lights, or are these restorations failing prematurely? Resin restorations are here to stay and many researchers have shown they can last just as long as amalgam restorations as long as proper techniques, materials, and technology are implemented.7,8 Successful resin restorations require proper polymerization, and with a little training and today’s improved LED curing light technology, can easily be accomplished.
References
1. Moore BK, Platt JA, Borges G, Chu TM, Katsilieri I. Depth of cure of dental resin composites: ISO 4049 depth and microhardness of types of materials and shades. Oper Dent. 2008;33(4):408-12.
2. Strategic Plan 2009–2013. Bethesda, MD: National Institute of Dental and Craniofacial Research, US Dept of Health and Human Services; 2009; p. 19; NIH Publication No. 09-7362.
3. Price RB, Felix CM, Whalen CM. Factors affecting the energy delivered to simulated Class I and Class V preparations. J Can Dent Assoc. 2010;76:a94.
4. Seth S, Lee CJ, Ayer CD. Effect of instruction on dental students’ ability to light cure a simulated restoration. J Can Dent Assoc. 2012;78:c123.
5. Segal P, Lugassy D, Mijiritsky E, et al. The effect of the light intensity and light distances of LED and QTH curing devices on the hardness of two light-cured nano-resin composites. Mater Sci Appl. 2015;6(11):1071-83.
6. Megremis S, Ong V, Lukic H, Shepelak H. An ADA Laboratory Evaluation of Light Emitting Diode Curing Lights. The ADA Professional Product Review. ADA website. http://www.ada.org/en/publications/ada-professional-product-review-ppr/archives/2014. Published November 2014.
7. Ferracane JL. Resin composite—state of the art. Dent Mater. 2011;27(1):29-38.
8. Opdam NJ, Bronkhorst EM, Loomans BA, Huysmans MC. 12-year survival of composite vs. amalgam restorations. J Dent Res. 2010;89(10):1063-1067.
Editor’s note: This article is supported by Ultradent.

Parag R. Kachalia, DDS, is the former vice chair of technology at the University of the Pacific. In 2017, he was selected as one of the Top 10 Young Educators in Dentistry in the United States by the Seattle Study Club. He is a fellow of the International and American College of Dentists. He has lectured internationally in the areas of technology, adhesive dentistry, cosmetic dentistry, photography, and dental materials. He maintains a private practice in San Ramon, California, with his wife, Dr. Charity Duncan.