Protecting dental staff from the most hazardous job in America

Andrew Barrett
John M. McMahon, DDS
In the January 2011 issue of Dental Economics, Paul Feuerstein, DMD, penned the article, “In the air tonight,” which discussed the harmful effects of poor indoor air quality in dental offices and solutions for indoor air quality improvement.1 Since that time, updated findings and new schools of thought have developed on the importance of cleaning dental office air as part of a proper infection control regime. This article will discuss these developments and present a brief case study.
A 2015 article in Business Insider identified the most damaging job to one’s health as that of a dental worker, which included dentists, dental hygienists, and dental laboratory technicians.2 The findings were based on analysis of the Occupational Information Network, a US
Department of Labor database with statistics on 974 occupations and 125 million employees. The dental profession ranked No. 1 based on high scores for exposure to contaminants and disease pathogens found in the air of dental offices.

Dr. John McMahon with Surgically Clean Air Cascade White air purifier.
Sources of indoor air contamination
In dental offices and dental laboratories, sources of indoor air contamination include the following:
- Bio-aerosols—Dental instruments create hazardous bio-aerosols containing microbes from the saliva, blood, and subgingival fluids. The dispersal of these fine droplets can remain suspended in the air for up to six hours.3 A toxic cloud spans from the floor to a height of six feet.3
- Patients—Sick patients can spread infectious illness throughout the office. Fine droplets that patients exhale can spread up to 160 feet from a patient’s mouth and travel up to 10 stories high through a building’s HVAC system.4,5,6,7
- Chemicals—There are many examples of chemical compounds in dental office air. For example, compounds from chemical disinfectants can affect staff, who face daily exposure to these pollutants. Mercury vapors can be dispersed in the air during removal of amalgam fillings. In labs, chemicals are an even bigger problem. Metal casting and porcelain baking can release dangerous airborne gases and vapors. In the creation of crowns, bridges, and dental prostheses, airborne contamination comes from metal alloys such as vironite, vitallium, wisil, and duralium. The most hazardous of them all may be methyl methacrylate monomer, which is used to generate polymer PMMA (polymethyl methacrylate). This compound is used in making dentures and other dental prostheses, as well as filters and cements.
- Dust—These particles come from many sources, most notably from carpet. Dust is an even bigger problem in the dental lab, as the grinding of materials creates a heavy airborne cloud of fine white dust.
Insufficiency of HVAC systems and PPE
Dental staff may believe they are protected from airborne contaminants and pathogens through a building’s heating, ventilation, and air conditioning (HVAC) system. Dr. Feuerstein, in his previously mentioned article, reveals the contrary. “Air conditioning systems do a great job of recirculating the air,” he says. “Bacteria, viruses, and all sorts of airborne things are being blown around the office.”1
Personal protective equipment (PPE) is also insufficient. The US Food and Drug Administration does not conduct or sponsor testing of surgical masks. In 2016, the Canadian Centre for Occupational Health and Safety stated:
- The filter material of surgical masks does not retain or filter out submicron particles.
- Surgical masks are not designed to eliminate air leakage around the edges.
- Surgical masks do not protect wearers from inhaling small particles that can remain airborne for long periods of time once they take off their masks and walk around their offices.6>


Figure 1: Test locations before and after air purification (30 days).
Air purification solutions
The following are selection criteria for helping identify efficacious air purification solutions.
Filtration—A system needs to remove air pollutants created in the dental office, which include dust, volatile organic compounds (VOCs), mold, bio-aerosols, bacteria, and odors. It should also kill bacteria and viruses using UV-C light. The Centers for Disease Control and Prevention (CDC) states, “If portable units are used, they should recirculate all the room air through medical grade filters.”7
Air-flow capacity—The amount of air that moves through a system is measured as cubic feet per minute (CFM). To provide the required efficacy, a system needs enough CFM to “turn over” the indoor air at least once every 30 minutes.7
Sound level—As air moves through an air purifier, it will generate sound. Too much sound will have a negative effect on those working near it. This usually results in the air purifier being turned down, which reduces the air-flow capacity and efficacy. A good air purifier should deliver a large enough air-flow capacity at a sound level of 50 dB. For reference, an average dishwasher operates at 50 dB, and human speech is 60 dB.
Air reenergization—There are those who believe that reenergizing indoor air can help people maintain a high level of cognitive function. Ion generators are thought to reenergize the indoor air. The belief is that breathing reenergized air can increase the flow of oxygen to the brain, resulting in higher alertness, decreased drowsiness, and more mental energy.8
Operational cost—Some units are inexpensive to purchase but have expensive consumables. Other systems are more expensive to purchase but have permanent components and cheaper consumables, so they are less expensive over time.
Effectiveness of air purifiers in dental offices
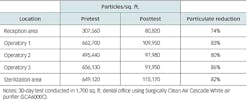
Research was conducted in the office of John M. McMahon, DDS, using the aforementioned selection criteria. An air-particle test was completed prior to installing a system, and it was repeated 30 days later (figure 1). There was a significant decrease in the airborne particulate throughout the office (table 1).
Table 1: Impact of stand-alone air purifier in a dental office
Conclusion
Studies in the Journal of Dental Hygiene,11International Journal of Dentistry,12Journal of the American Dental Association,13British Dental Journal,14 University of Athens,15 the SRM Journal of Research in Sciences Dental,16 and Tsinghua University Bejing17 are recommending a new school of thought on the use of medical-grade air purifiers in managing the dangers of indoor dental office air. Dental workers breathe 11,000 L of indoor air a day;18 take the time to protect yourself, your staff, and your patients with clean, pure, and reenergized air.
References
1. Feuerstein P. In the air tonight. Dental Economics website. http://www.dentaleconomics.com/articles/print/volume-101/issue-1/technology-needs/in-the-air-tonight.html. Published January 1, 2011. Accessed September 1, 2017.
2. Kiersz A. The 27 jobs that are most damaging to your health. Business Insider website. Published November 2, 2015. Accessed October 1, 2017.
3. Zeisler J. Cleaner air in the dental office. Ontario Dentist. 2009;9:28-29.
4. Welty S. Airborne influenza in dry wintertime indoor air [slideshow presentation]. https://tc0906.ashraetcs.org/documents/programs/Steve_Welty_CIAQ_Flu_2_13_2013_Revised_1_24_2015.pdf. Presented February 13, 2013. Updated January 24, 2015. Accessed October 1, 2017.
5. Yu I, Li Y, Wong TW, et al. Evidence of airborne transmission of the severe acute respiratory syndrome virus. New Engl J Med. 2004;350:1731-1739.
6. Welty S. How far can airborne viruses travel? Scribd website. https://www.scribd.com/doc/257678796/how-far-do-airborne-pathogens-travel. Accessed October 1, 2017.
7. Kopman J. Sneezed germs travel how far? The Weather Channel Website. https://weather.com/health/news/how-far-does-your-sneeze-travel-20140410. Published April 10, 2014. Accessed October 1, 2017.
8. Hardie J. Why face masks don’t work: A revealing review. Oral Health website. https://www.oralhealthgroup.com/features/face-masks-dont-work-revealing-review/. Published Oct 18, 2016. Accessed October 1, 2017.
9. U.S. Department of Health & Human Services Centers for Disease Control & Prevention (CDC)
10. Howard PJ. The Owners Manual for the Brain. Bard Press: 2006.
11. Jacks ME. A laboratory comparison of evacuation devices on aerosol reduction. J Dent Hyg. 2002;76(3):202-206.
12. Leggat PA, Kedjarune U. Bacterial aerosols in the dental clinic: a review. Int Dent J. 2001;51(1):39-44.
13. Godwin CC, Batterman SA, Sahni SP, Peng CY. Indoor environment quality in dental clinics: potential concerns from particulate matter. Am J Dent. 2003 Aug;16(4):260-266.
14. Hallier C, Williams DW, Potts AJ, Lewis MA. A pilot study of bioaerosol reduction using an air cleaning system during dental procedures. Br Dent J. 2010;209(8):E14.
15. Helmis GC, Tzoutzas J, Flocas HA, et al. Indoor air quality in a dentistry clinic. Sci Total Environ. 2007;377(2-3):349-365.
16. Yadav N, Agarwal B, Maheshwari C. Role of high-efficiency particulate arrestor filters in control of air borne infections in dental clinics. J Res Med Sci. 2015;6(4):240-242.
17. Chen C, Zhao B, Cui W, Dong L, An N, Ouyang X. The effectiveness of an air cleaner in controlling droplet/aerosol particle dispersion emitted from a patient’s mouth in the indoor environment of dental clinics. J R Soc Interface. 2010;7(48):1105-1118.
18. Adams WC. How much air do we breathe? https://www.arb.ca.gov/research/resnotes/notes/94-11.htm. California Environmental Protection Agency Air Resources Board website. Published August 1994. Accessed October 1, 2017.

Andrew Barrett is a graduate of the Wilfrid Laurier University Business School. He has more than 25 years of business experience working for global consumer goods companies and global electronic manufacturers. He is chief marketing officer for Surgically Clean Air Inc.

John M. McMahon, DDS, is a fourth-generation dentist. He graduated from the University of Michigan with an undergraduate degree in brain behavior and cognitive science, followed by a doctorate in dental surgery. Dr. McMahon was recently named one of America’s Top 40 Under 40 Best Young Dentists in Incisal Edge magazine.