Ask Dr. Christensen
In this monthly feature, Dr. Gordon Christensen addresses the most frequently asked questions from Dental Economics® readers. If you would like to submit a question to Dr. Christensen, please send an e-mail to [email protected].
For more on this topic, go to www.dentaleconomics.com and search using the following key words: tooth-colored, onlays, inlays, dental codes, composite resins, polymerization, low shrink, restorative materials.
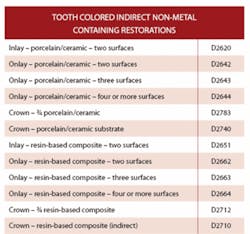
Q Tooth-colored onlays and inlays are being promoted in many continuing education programs and articles in professional journals. Are these restorations really serving adequately, and if so, are third-party payment programs offering benefits for them?A The number of full crowns placed in the U.S. is amazing. Estimates are that more than 40 million crowns are placed annually in the United States. Are all of these crowns placed for functional reasons? The obvious answer is no. Many of them are being placed for esthetic reasons. Would the esthetic result be better with more conservative restorations instead of crowns? Yes, an onlay or inlay made from tooth-colored material can be a longer-lasting restoration from an esthetic standpoint, since gingival recession on a tooth restored with an onlay or inlay only shows the patient's natural tooth structure instead of an objectionable crown margin. Also, when placed in early adulthood, these more conservative restorations still leave the potential for more aggressive full crowns to be placed later in life. I feel strongly that tooth-colored onlays and inlays should be placed more, and that full crowns should be placed to a lesser degree.There are ADA codes for these restorations as follows:

Although there are code numbers for these restorations, does that mean that third-party payment companies will pay for these restorations? The popularity of chairside milling devices such as CEREC® from Sirona and E4D™ from D4D Technologies LLC has popularized conservative onlay and inlay restorations, and third-party payment companies have recognized that they are serving well when placed at an adequate level. Internationally available clinical research supports that finding.

Whether the onlay or inlay is made by a chairside milling device or a dental laboratory technician, the previously stated code numbers are the same. An onlay, by definition, must cover at least one cusp of the tooth. Many companies are paying for restorations identified as an onlay or a ¾ crown.

They may offer only the lower level direct resin-based composite or amalgam reimbursement for the inlay designations. Patients should be advised of the potential lack of higher level payment for those restorations designated as inlays.

Both ceramic and polymer restorative materials are being used for these restorations. Ceramic, mainly pressed ceramic such as IPS Empress from Ivoclar Vivadent, are used most (see Figures 1 and 2). Both laboratory technician-made and machine-milled restorations are popular.
Although the success of gold alloy restorations is well-known, most patients prefer tooth-colored restorations. It is comforting to recognize that properly made and cemented tooth-colored onlays and inlays are serving well and that they satisfy that demand.
See our new video on tooth-colored onlays and inlays. It includes close-up demonstrations of tooth preparations, impressions, cements, bonding agents, and nonsensitive, predictable cementation. It is an excellent technique guide for both dentists and dental assistants, and is a great aid for those who are currently incorporating this technique into their practices.
For more information on V1529, “Esthetic Alternatives for Crowns — Tooth-Colored Onlays and Inlays,” contact Practical Clinical Courses at (800) 223-6569 or visit our Web site at www.pcdental.com.
Q I have heard that the new low shrinkage composite resins are better than previously available resins. What are the potential advantages of low shrinkage restorative resins?A Shrinkage has always been a real or imagined challenge when using restorative resins. Some of the first polymethyl methacrylate restorative resins that were present in the 1950s and 1960s were Sevriton and Bonfill. These resins had high shrinkage during polymerization of about 6%. The real and proposed problems associated with this amount of shrinkage are stress in the cavity preparation and marginal openings on finishing, commonly named a “white line” by clinical dentists. Polymerization shrinkage has remained as a challenge, with the resin-based composite restorative resins of today shrinking about 2% and flowable resins shrinking up to 5% during polymerization, depending on brand name. Several companies are planning on bringing “low shrink” resin-based composite materials to the profession.The new products coming out have reported shrinkage of about 1%, which will be significantly less than previously available resin-based composites. These restorative materials represent a departure from the resin formulations used for the past 50 years, and several years of clinical observation will be necessary to determine their clinical characteristics during service.

The first brand to appear is Filtek™ LS Low Shrink Posterior Restorative System from 3M ESPE (photo at right). This resin uses silorane chemistry instead of the well-known bis-GMA or urethane dimethacrylate chemistry that has been used in almost all resin-based composite dental restorative resins. The new resin restorative material has increased working time even when in the operating light. This characteristic will be an advantage in some clinical situations.
A special adhesive system is necessary for use with Filtek LS, the LS System Adhesive Self-Etch Primer, which is used before the LS Bond. The need for a specific bonding system may be a disadvantage for the product, since most clinicians use more than one brand of resin restorative material. The company has aimed this radiopaque product at typical posterior tooth restoration needs. There are four colors available in capsules or syringes.
The obvious question is what advantages will a typical dental clinician receive when using a low shrinkage resin? Many scientific studies have been aimed at the real and proposed problems with resin shrinkage during polymerization. In my opinion, most of them appear to have minimal clinical significance.
The two most potentially problematic situations relative to excessive polymerization shrinkage are: stress in the tooth preparation created by the shrinkage with alleged cracks in the tooth, or continuing ongoing stress that could potentially relate to subsequent tooth or restoration failure; and the development of an opening of restoration margins during finishing procedures.
Clinicians are familiar with the development of a “white line” around restorations during finishing. Often, the resin looks excellent when initially placed, and then the white line occurs as finishing is accomplished. This phenomenon occurs commonly as burs that are nonconcentric are used on margins, or rotary discs are used too aggressively on margins. However, in my experience, use of new, sharp, concentric burs and/or nonaggressive use of disks during finishing can prevent the development of the white line phenomenon.
Is the white line a clinical problem? If the white line is located on a margin that is visible when the patient smiles, it may be a slight esthetic problem. More research is needed to determine if the white line is more conducive to future dental caries. Since the white line is a microscopic crevice between tooth structure and the restorative material, logical thinking would conclude that the tooth would be more susceptible to recurrent dental caries in the white line area.
The conclusive answer to your question is not easy at this time. Low polymerization shrinkage resin-based composites have the potential to reduce stress in teeth and to create fewer minute cracks and subsequent restoration failures. In my opinion, based on personal placement of many resin-based composite restorations and research observation of the “white line” under significant magnification, the main clinical difference clinicians will observe is fewer white lines during finishing. The profession should welcome the advent of “low shrink” resin-based composites, and research will continue to show their advantages. At this time, their initial-use characteristics look very promising.
Dr. Christensen is a practicing prosthodontist in Provo, Utah, and Dean of the Scottsdale Center for Dentistry. He is the founder and director of Practical Clinical Courses, an international continuing-education organization initiated in 1981 for dental professionals. Dr. Christensen is a co-founder (with his wife, Rella) and senior consultant of Clinicians Report (formerly Clinical Research Associates), which since 1976 has conducted research in all areas of dentistry and publishes its findings to the dental profession in the “Gordon J. Christensen Clinicians Report” monthly newsletter. Dr. Christensen has educational videos and hands-on courses on the above topics available through Practical Clinical Courses. Call (800) 223-6569 or (801) 226-6569.