The Many Happy Returns of 3–D Imaging


by Jeffrey H. Brooks, DMD
With a primarily implant–based practice, our practice implemented cone beam CT (CBCT) technology in early 2005. Since that time, we have witnessed a positive and expeditious return on investment (ROI), both directly and indirectly.
For more on this topic, go to www.dentaleconomics.com and search using the following key words: 3–D imaging, cone beam CT, implant–based, ROI, Dr. Jeffrey Brooks.
With a primarily implant–based practice, our practice can easily be categorized as a high–end user of 3–D imaging. Prior to using cone beam technology, all treatment–planning data was derived from a clinical exam, 2–D panoramic radiographs — with obvious magnification artifact, periapical radiographs, and occasionally with tomography. While 2–D imaging is sufficient for many dental–related procedures, 3–D cross–sectional imaging has become the standard of care for evaluating the implant recipient site both qualitatively and quantitatively.
Without the detailed information that a 3–D scan provides, multiple treatment plan contingencies often must be presented to patients. Presenting multiple unnecessary contingency plans can result in a patient's loss of confidence in the practitioner's ability to present a concise diagnosis and treatment plan. With CBCT technology, a more concise treatment plan can indeed be presented to the patient initially, which results in higher patient confidence levels relating to the proposed treatment. With a cone beam scan, you can clearly demonstrate to the patient areas of insufficient bone at the recipient site and whether bone grafting will be necessary prior to implant placement. When this definitive information is presented to the patient, we have noted in our practice, treatment acceptance increases substantially. We have attributed this benefit to the substantial increase in implant numbers that our practice has appreciated since instituting this technology.

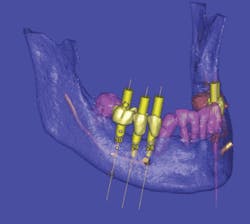
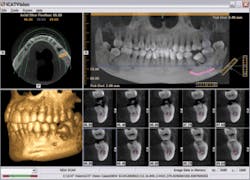
A patient with a previously grafted alveolar cleft was recently referred to our clinic by another surgical practitioner for implant placement. While the referring practitioner indicated that the grafted area was an acceptable recipient site based on available 2–D imaging, the cone beam scan showed grossly insufficient bone into which to place the implant. This is clearly evident on the images (Fig. 1, 2). If implant surgery had been instituted based on the information provided by the 2–D images, without this additional and vital information, the patient's confidence could have been lost, as well as potential referrals to his friends and family, possibly causing a negative impact to ROI. In this case, however, a 3–D computer model clearly pointed out the bony deficiency prior to surgery.

Specialized 3–D reconstructive software also allows practitioners to provide 3–D images and viewer software to the referring dentist, allowing for collaboration regarding positioning, placement, and angulation of implants prior to surgical placement procedures (Fig. 3).
Practitioners clearly gain another layer of respect from their referring dentists and patients when they take the extra step of obtaining the highest quality diagnostic technology and implementing this in their practices. Our practice witnessed an almost 150–implant increase the first year and a 200–implant increase in the second year after implementing cone Beam (i–CAT®) technology, essentially covering the cost of the initial investment during the first year.
A direct form of ROI is gained from the many applications of the scans depending on the type of practice. An orthodontist can obtain multiple radiographic studies by taking one 3–D scan and extracting a panoramic, a cephalometric, or a 3–D reconstruction, as well as multiple other radiographic views from this one radiographic study. For example, if a typical orthodontist with approximately 100 new cases a month charged $300 a scan, in less than a year this practitioner could potentially pay for this equipment. Dentists placing implants may have fewer cases per month, yet receive their biggest return on investment through case acceptance, especially with larger cases — a more indirect, but very effective and expeditious ROI.
Since 3–D imaging is available in both full and partial fields of view, it is wise to discuss individual needs with a sales representative. General dentists, periodontists, and endodontists rarely need greater than a partial field of view, which reduces the initial investment and possibly some liability concerns, thus yielding a faster return (Fig. 4). For these dentists, a system with a scan field that captures the arches, the possibility for expansion to the TMJ region, and the ability to double as a traditional 2–D pan, may boost not only the rate of return on investment, but increase the myriad of options to the practice.
Orthodontists and oral surgeons often need the extended field of view for cephalometric radiographs and orthognathic treatment planning, and viewing cranial facial deformities, pathology, and trauma (Fig. 5). It is important to note that with a fully extended field of view scan, the dentist is responsible for interpreting or having someone else interpret the scan to detect pathology within the confines of the scan. It is not sufficient from a liability standpoint to address the dental issues alone.

Our clinic has adopted the protocol of taking a scan for every implant case prior to surgery as the standard of care. An official report by American Academy of Oral and Maxillofacial Radiology1 notes that panoramic imaging alone is not sufficient for providing all of the necessary information described for optimal implant selection, and should be augmented by either tomography or a CT. As a result, as it relates to both direct and indirect ROI, cone beam imaging pays for itself and brings a new level of clarity to both the doctor and the patient.
References: 1. Parameters of Radiological Care. Oral Surgery/Oral Medicine and Oral Pathology Journal, Volume 91, Number 5, May 2001.
Dr. Jeffrey H. Brooks has been in private oral surgery practice in Little Rock, Ark., for the past 16 years. He is an assistant professor at the University of Tennessee Department of Oral and Maxillofacial Surgery, Memphis, Tenn. Dr. Brooks is a well–respected author and lecturer, and frequently presents the "Benefits of Cone Beam Technology in the Dental Practice" for Imaging Sciences International. Reach him at drbrooks@dds–i.com.