How robotics quadrupled my practice's implant volume

Haptic robotics significantly improves accuracy, visualization, and flexibility during dental implant procedures.1,2 From an economic perspective, robotics adds value by simplifying difficult procedures and increasing the volume of implants performed. While profitability varies due to a number of factors, it is generally accepted that placing implants, particularly in a single stage (i.e., placing the implant as well as the transmucosal abutment at the same time), is a profitable procedure.3 Approximately 36 million Americans do not have any teeth, and 120 million people in the US are missing at least one tooth. With the aging demographic in this country, these implant numbers are only expected to grow.4
Related reading:
- Learn about the next game-changer in your practice: Robotics
- Moving from surgical guides to robotics: A no-brainer
In my entire residency, I placed about 75 implants. For single implants, I used freehand techniques; however, if there were multiple, I used preprinted surgical guides. Before integrating robot-assisted surgery into my practice, I used mostly freehand techniques for dental implants with the occasional surgical guide, as I’ve found that surgical guides don’t always fit well, resulting in suboptimally placed implants. I’ve found this to be especially true in edentulous cases where the guides are tissue-borne. These issues are well documented, not unique to my practice.5
In 2017, the Food and Drug Administration (FDA) cleared the Yomi system (Neocis) as the first robotic system for dental implant procedures. While I maintain control of the handpiece, the robot haptically guides the location, orientation, and depth of both the bone preparation and implant placement. This guidance is driven by the preoperative plan I create based on a CBCT scan.
There are many benefits to using a robotic system. Surgical guides are no longer necessary, but the significant accuracy of placement allows me to avoid critical structures and optimize the available bone. With robotics, I can perform same-day surgery, and I’m free to adjust the surgical plan intraoperatively. There’s no need for complicated surgical kits or guide sleeves, and I have an unobstructed view of the operative site during the procedure. Most importantly, Yomi is an open platform that allows me to use any implant system I choose.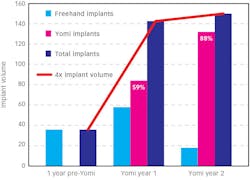
I recently looked at my implant volume from the year before I integrated robotics into my practice compared to the first and second year following adoption of robotics (figure 1). The year before I adopted robotic technology, I performed a respectable 36 dental implants, all freehand. The year after I started doing robotic surgery, my implant volume quadrupled to an impressive 142 implants! During this first year, 59% of my implants were placed robotically. At the time, the robot was only cleared for partially edentulous patients with a tooth-borne fiducial splint, so I was still performing freehand implants on fully edentulous patients. A few months into my second year of robotic dental implant placement, the FDA cleared a bone-mounted, transmucosal splint for edentulous patients. While my overall implant volume did not increase significantly (likely because of COVID-19), the percentage of implants placed robotically grew to 88%.
Adopting robotic implant placement into my practice has provided several advantages. Economically, my yearly implant volume quadrupled for a highly profitable procedure. Clinically, the technology makes routine cases incredibly simple and efficient. For complex cases, the benefits grow exponentially. For example, some patients present with limited vertical height (e.g., 5 mm or 6 mm) directly above a maxillary implant site. Unfortunately, it’s not uncommon to perforate the sinus membrane when preparing the osteotomy freehand. With this type of patient, I might offer a sinus lift and then need to wait four to six months for healing before implanting freehand. With robotics, I can place the implant and elevate the sinus at the same time by planning a short implant. This way, the robot physically stops me at the appropriate depth so I can tap the sinus floor up and not create an oroantral communication. Robotic assistance has boosted confidence, flexibility, safety, and accuracy on my implant cases, all while significantly growing my business.
Editor's note: This article appeared in the November 2021 print edition ofDental Economics.REFERENCES
- Rawal S, Tillery DE Jr, Brewer P. Robotic-assisted prosthetically driven planning and immediate placement of a dental implant. Compend Contin Educ Dent. 2020;41(1):26-31.
- Bolding SL, Reebye UN. Accuracy of haptic robotic guidance of dental implant surgery for completely edentulous arches. J Prosthet Dent. 2021;S0022-3913(21)00056-1. doi:10.1016/j.prosdent.2020.12.048
- Jones JP, Ellis E 3rd. Are office-based oral and maxillofacial surgical procedures profitable? A benefit-cost analysis. J Oral Maxillofac Surg. 2019;77(11):2205-2214. doi:10.1016/j.joms.2019.05.015
- Dye B, Thornton-Evans G, Li X, Iafolla T. Dental caries and tooth loss in adults in the United States, 2011-2012. NCHS Data Brief. 2015;(197):197.
- Unsal GS, Turkyilmaz I, Lakhia S. Advantages and limitations of implant surgery with CAD/CAM surgical guides: a literature review. J Clin Exp Dent. 2020;12(4):e409-e417. doi:10.4317/jced.55871
Bradley Pinker, DDS, MD, is a board-certified oral and maxillofacial surgeon. He earned his doctor of dental surgery degree from Columbia University College of Dental Medicine in New York City, New York, trained in oral and maxillofacial surgery at the University of North Carolina at Chapel Hill, and earned his doctor of medicine degree from the University of North Carolina at Chapel Hill. His professional interests include orthognathic surgery, robot-assisted dental implant surgery, dentoalveolar surgery, maxillofacial pathology, and maxillofacial trauma.
About the Author

Bradley Pinker, DDS, MD
Bradley Pinker, DDS, MD, is a board-certified oral and maxillofacial surgeon. He earned his doctor of dental surgery degree from Columbia University College of Dental Medicine in New York City, New York, trained in oral and maxillofacial surgery at the University of North Carolina at Chapel Hill, and earned his doctor of medicine degree from the University of North Carolina at Chapel Hill. His professional interests include orthognathic surgery, robot-assisted dental implant surgery, dentoalveolar surgery, maxillofacial pathology, and maxillofacial trauma.
Updated October 6, 2021