Ask Dr. Christensen

by Gordon J. Christensen, DDS, MSD, PhD
In this monthly feature, Dr. Gordon Christensen addresses the most frequently asked questions from Dental Economics® readers. If you would like to submit a question to Dr. Christensen, please send an email to [email protected].
Q I have had a few clinical situations in which the screw holding an abutment in place on an implant has come loose during service, and I could not get the cemented crown off to retighten the screw. What are my alternatives to avoid this frustrating occurrence in the future?
A This is a relatively frequent occurrence in the profession. I have conducted surveys on this topic with continuing education course attendees and have found that about 10% to 15% of screw-retained abutments placed over implants come loose after a few years in service. That doesn't sound like many problems, but when you're the dentist with the problem, it is time consuming and expensive to correct a situation that patients do not understand or appreciate. I will provide several methods to reduce or eliminate the clinical problem.
Screw going directly through the occlusal surface of the crown and into the implant
This type of crown attachment to an implant is currently uncommon. However, use of this technique is very easy, and it will overcome the problem of retightening the screw when an implant screw comes loose.
As you know, screw attachment of the crown to the implant usually requires a "patch" on the occlusal surface of the crown to fill the hole in the crown. The appearance of such closure of the screw hole can be unacceptable for some esthetically sensitive patients. However, the hole can be filled esthetically if you have appropriate materials.
I suggest the following porcelain repair kits as example products -- Bisco Intraoral Repair Kit and Ultradent Porcelain Repair Kit. Both kits have the necessary components to etch ceramic, cover metal with opaque resin, bond to the ceramic, and effectively block out the objectionable hole. These same kits can be used to similarly fill an endodontic access hole in a ceramic or porcelain-fused-to-metal crown.
Assuming the screw that goes entirely through the crown becomes loose in service, what do you do? You remove the composite filler in the occlusal surface of the crown, remove the screw, clean the screw hole and the screw, and tighten the screw back into place. The occlusal hole must again be filled adequately. This entire procedure requires only a few minutes.
In recent months, laboratory technicians have reported to me that more dentists than ever before are using this technique to simplify the tightening of screws when they come loose.

Use weak cement to lute the crown to the abutment that is screwed to the implant
This is one of the more popular techniques to allow a relatively easy method to remove the crown from the abutment and tighten the loose screw. Here is a list of the steps in cementing a crown over an implant abutment with the abutment screwed to the implant.
- Securing and cementing an implant abutment and implant supported crown
Make sure the abutment seats adequately on the implant. - Torque the abutment retaining screw to ~35 Ncm.
- Place a "hard" cotton roll over the implant abutment (no crown on it), and have the patient chew on the cotton roll with force while you do something else for 5 to 10 minutes.
- Return to the patient and again torque the screw. It will go farther into the screw hole, often one quarter to one half turn more.
- Remove the screw.
- Place a cleaning solution into the screw hole and wash it out.
- Clean blood, saliva, or other contaminants from the screw.
- Place sealer (Preat Ceka Bond) on the screw.
- Again, place the screw into the screw hole and torque it to ~35 Ncm into place.
- Seat the crown with Premier Implant Cement or other weakened resin cement, placing cement only on the apical half of the internal of the crown so it can be removed in the future if necessary.
- Clean all cement residue from the juncture of the abutment and the crown!
The above technique is one I use routinely with success. It reduces the disagreeable screw loosening that all of us have experienced.

What should you do in the event that the screw still comes loose in spite of your best efforts?
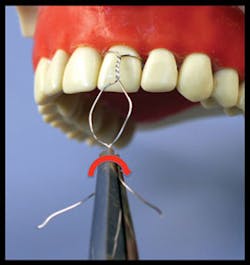
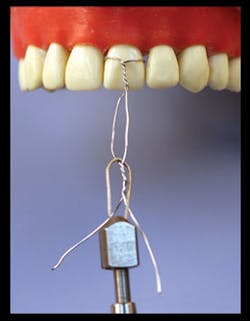
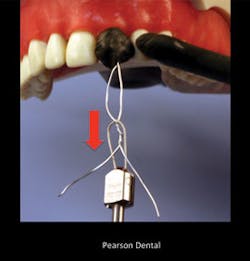
Figs. 1 to 7 show the technique that is almost always successful to remove the crown from the abutment. This technique will successfully remove the crown, assuming you did not use "permanent" cement. It will allow you to retighten the screw after the crown has been removed. Although it seems somewhat objectionable to the patient to tap on their crown in the manner shown in the images, the result is positive for both the dentist and patient.

What to do if you cannot tap the cemented crown off the implant
Many dentists become frustrated when the crown cannot be removed using any method. The next alternative is to make an access hole in the occlusal surface of the crown extending into the screw hole. It is important that the dentist who cemented the crown over the abutment used a soft material to fill the hole leading to the abutment screw. Among the adequate materials to fill the screw access hole are gutta percha, cotton, impression material, and plumber's tape.
Assuming a soft material has been used, making the hole in the occlusal surface of the crown will usually allow you to easily find the screw hole. Remove the soft material. Remove the loose screw. Clean the screw hole and the screw. Place Ceka Bond from Preat Corp. or a similar product on the screw to seal it and provide slightly better resistance to it loosening again, and screw it into place. Seal the access hole as described previously.

If you have penetrated a ceramic crown to accomplish this procedure, you have probably weakened the ceramic, and I suggest warning the patient of potential crown failure.
Use of implant systems using a Morse taper or a screw and a Morse taper
Several current implant systems use a Morse taper on the abutment-implant connection, which is a slight taper on the abutment projection leading into the implant that is matched with the implant internal surface. It has been reported that these systems have a better probability to reduce the implant abutment coming loose from the implant body.
Additional information
Our organization, Practical Clinical Courses, has additional educational information for you on this and related subjects.
- Our video, V1961, How to Repair and Maintain Fixed Restorations, shows the technique described for crown removal as well as many other repair techniques.
- Additionally, several two-day related courses are presented in Utah. Examples are:
> Successful, Real-World Practice – Fixed Prosthodontics
> Christensen Comprehensive – Affordable Treatment of Complex Cases
For information, go to www.pccdental.com or call (800) 223-6569.
Summary
Abutment screws come loose occasionally. The previous information provides some alternatives for you. Use your own judgment to determine which of the techniques best fits your clinical needs.
Gordon Christensen, DDS, MSD, PhD, is a practicing prosthodontist in Provo, Utah. He is the founder and director of Practical Clinical Courses, an international continuing-education organization initiated in 1981 for dental professionals. Dr. Christensen is a cofounder (with his wife, Dr. Rella Christensen) and CEO of CLINICIANS REPORT (formerly Clinical Research Associates).
Past DE Issues