The economics of the digital dental record: Can you afford not to make the switch?
By Bradley A. Dykstra, DDS, MBA
For more on this topic, go to www.dentaleconomics.com and search using the following key words: economics of digital dental records, electronic medical records, Dr. Bradley Dykstra.
Are you still on the fence about the cost effectiveness of transitioning from the traditional way of maintaining dental patient records to the truly electronic or digital patient chart? Are you confused about what digital charts are? Are they really possible, and if so, how much do they cost?
First of all, it is well documented that it is very possible to have totally electronic patient charts since many dentists successfully do so. The technology — both hardware and software — is now well developed. (We will refer to these digital charts as EMRs, for Electronic Medical Records.)
It is important to understand that in a few years, the government will require that all patient medical and dental records be in digital format. It is natural to think that purchasing EMRs is too expensive, but this is a shortsighted approach based on the faulty assumption that the current way of doing things is free.
Believe it or not, the status quo is not free, and is in fact very costly. This article will examine what is needed to make the transition, and will highlight a few of the hidden costs of not making the switch.
What is the dental EMR?
The dental EMR is everything that is now in the traditional paper chart, maintained in a digital format. The EMR includes the patient personal registration information, insurance information, medical and dental history and any updates, clinical chart and progress notes, radiographs, photographs, and any correspondence with specialists, other dentists, or health–care professionals.
The hidden costs
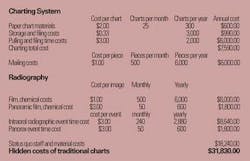
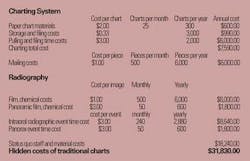
The first hidden cost is in constructing, using, and storing the paper clinical chart. The materials for every new chart cost a minimum of $2. If your office has 300 new patients a year, that's an ongoing cost of $600 a year. Purchasing file cabinets, the square footage floor costs for them, and the long–term storage of old records adds another $1,000 a year (33 cents per chart for 3,000 charts).
Printing and mailing documents — such as insurance forms, recall or reminder cards, correspondence to other clinicians, and patient newsletters — is also a large hidden expense. By the time postage, paper, cards, envelopes, and time are added up, costs approach $1 per piece. If you normally send 1,000 pieces of mail a month and reduce the number of documents prepared and mailed by 50% using e–mail, it will result in a monthly savings of $500 per month, or $6,000 per year.
Staff time is another large monetary drain. Time is spent putting a chart together, pulling it every time a patient calls or comes in, pulling it to correspond with specialists or file insurance EOBs, and then refiling it. Add the time wasted looking for misfiled or lost charts. On average, a conservative estimate is six minutes per chart per year. If the total hourly cost of employing the staff person is $30 per hour (50 cents per minute), this adds $3 per active patient chart per year. If you have 2,000 active patients, that equals $6,000 per year. The grand total so far is at least $7,590.
The biggest hidden cost is in radiographics. The first obvious cost savings is no longer purchasing film, chemicals, and mounts, no longer maintaining the processor, and no longer disposing of the hazardous chemicals. The average total cost per film of the traditional system is approximately $1 per film, more if double film packets are used.
If your office averages 500 films a month, including retakes, this is a savings of $500 per month, or $6,000 a year. The cost of the film and chemicals for developing a panorex is $3. If your office averages 50 per month, that is another $150 cost per month, or $1,800 per year.
The biggest hidden cost savings is time. The image is visible in two to three seconds, not six to 10 minutes. To calculate your savings, count the number of times radiographs are taken on patients during the day. Count each series, regardless of the number of films, as an event. Next, assign a conservative time allowance of six minutes per event to allow time for processing and mounting. Remember to count any retake.
Using the same conservative cost per minute of employee time (hygienist or assistant), this equals $3 per radiographic event. If there are 15 events per day between doctor and hygiene, this equals $45 per day in hidden costs. For a 16 workday month, this adds up to $720 a month, or $8,640 a year.
Another benefit is that if a retake is necessary, the tube head, sensor, and lead apron are still in position, so it is easy to reposition and correct the error. This is much more efficient and effective than guessing what's wrong and hoping to get the angulations correct the second time. This saves at least five minutes for every retake.

Opportunity cost is a term that needs clarification. Opportunity cost, or economic opportunity loss, is the value of the next best alternative foregone as the result of doing something else. In the practice setting, it is the cost of the time taken for one task (time for traditional charts, photography, and radiography) that prevents a person from doing another more productive procedure.
In my office, the time saved with digital radiography allows each of my hygienists to see one more patient per day without working any harder, just smarter. With two or three hygienists working per day and an average hygiene visit cost of $110, this equals an increased daily production of $200 to $300, or $1,000 a week.
Digital photography makes documentation of dental conditions virtually free. There is no film or developing cost, and any unacceptable images can be deleted and retaken in just a few seconds. These photos are not only invaluable for patient education and treatment acceptance, but also for legal and insurance documentation.
Now let's examine the doctor's time schedule. If you take a minimum of three films for an endodontic procedure with a time savings of five minutes per film, this cuts 15 minutes off an endodontic procedure. If the doctor's production goal is $400 per hour, this opportunity can equal a $100 hidden cost.
If one endo procedure per day is completed and there are 16 workdays per month on average, this is an opportunity cost of $1,600 per month, or $19,200 per year. For emergency patients, there is a minimum of a five–minute time savings, or a hidden cost of $33 per patient. Again, one per day with 16 workdays per month results in a time savings of $528 per month, or $6,336 annually.
The additional advantage of never having to duplicate radiographs or photographs to forward them to insurance companies, specialists, or subsequent treating dentists also saves costs on materials and time. Radiographs can simply be electronically forwarded to the desired destination.
Looking at the big picture, it becomes obvious that maintaining the traditional dental chart is not free. In fact, it is very costly. Many of the other benefits of the digital record are clearly documented in other articles, but looking strictly at the dollars and cents as outlined in the table should give you a new perspective on the long–term investment in your practice. Plug your own numbers into the table and see what you're leaving on the table.
Dr. Bradley Dykstra is a general dentist in private practice in Hudsonville, Mich. He is a graduate of the University of Michigan's dental school and received his MBA from Grand Valley State University. Dr. Dykstra speaks on integrating technology into the dental office, and consults through his company, Anchor Dental Consulting. Reach him at (616) 669–6600, or e–mail [email protected].