How ClearChoice came to be in the dental profession

My private dental office in Denver was the perfect place to start a new experiment in implant dentistry—or at least, that was what I had been told. I would be inserting dental implants for patients, who’d then be chauffeured to another office for placement of fixed-denture prostheses. I would simply squeeze the patients into my already busy daily schedule, or work through lunch or late to get them done. After all, how many patients could there be?
My office manager suggested we open up a few half-hour slots in the schedule, so if no one showed, we would not expend too much schedule time. Our faith in the process of advertising for dental implant patients was extremely low. In fact, I hardly thought about it until about a week before, when suddenly we became double-booked and I started to worry that people would actually show up for their scheduled surgeries. What made the schedule doubly difficult was consulting with the patient just prior to surgery, the patient having had initial consult from the prosthetic treatment team.
At the end of the first month, my already extremely busy implant practice doubled its production. Work hours and office stress increased exponentially. And now, the future schedule was already jammed. We suddenly realized there was no end in sight. Something had to give.
This was the first month of ClearChoice. The surgeon, the prosthodontist, the lab, the call center, and supporting management were spread out all over town.
As a dentist who had never had an association with corporate dentistry, this was extremely unsettling to me and made me second guess my decision to give this new idea a try. But for some reason I kept going and eventually settled into a well-organized routine. Also, a strange thing happened. We suddenly realized we absolutely loved what we were doing. The patient experience and transformation were amazing, and it was transforming us.
Four months later, the entire team moved into a new centralized office. Kevin Mosher, future CEO of ClearChoice, attended our grand opening as president of Nobel BioCare. Over the years, the headquarters office was visited by thousands of professionals trying to understand what had just happened to implant dentistry.
You might also be interested in
Implant dentistry: The next DSO darling
3 dentists offer expert case acceptance advice
Dental Economics sparks the idea
Interestingly, the idea of ClearChoice came from this very magazine, Dental Economics, which in 2001 ran a cover story on immediate loading of dental implants. A few practitioners had tried immediate loading for complete-arch treatment and it had worked, and Dental Economics reported this story—perhaps the most important story of our time in dentistry.1,2
Dr. Don Miloni was a general dentist who had particular skill in complete dentures and had popularized denture clinics in Omaha, Nebraska. He had a long history of trying to satisfy atrophic edentulous patients with dentures, so when he saw the magazine describing implants fixing a denture into place, it hit him like a bolt of lightning. The concept of ClearChoice flashed into his mind in that instant.
Miloni needed legal and business expertise to help formulate the idea and express it in a viable business plan. He found that in Steve Boyd, an international business executive with multimedia marketing expertise, and Bobby Turner, a prominent Denver attorney. They formed a partnership and enlisted a specialized attorney, Brian Caleo, to form a dental service organization (DSO) in which doctors could self-direct their practice of dentistry but receive management services from the management team. Attorney Dan Christopher provided a regulatory role, especially important as the clinic system expanded across the nation.
One day Miloni and Boyd approached me in the parking lot of the church we all attended and told me about their idea for a chain of dental implant centers. I initially dismissed this idea out of hand. They persisted, approaching me five times before I finally accepted.
One of the first orders of business was to hire marketing specialist Larry Deutsch, who had brought LASIK to market in Canada and had particular expertise in thematic advertising to attract potential patients.
Once the executive team was formed, Steve Boyd asked, “Who in the world is doing this?” The answer was “No one in the United States.” There was, however, one doctor in Lisbon, Portugal, who did, and that was Dr. Paulo Maló. So Boyd, Miloni, and Deutsch flew to see Dr. Maló. This would be one of many visits to Portugal to learn from Maló and his associate-bioengineer, Bo Rangert, about something they called the “all-on-four.”3
In business, as in dentistry, it is difficult to swallow one’s pride. In a startup venture, everyone seems to have their own ideas as to how best to do something, and so it was with ClearChoice. For example, nearly every dentist seemed to have “a better idea” for how to perform complete-arch treatment, a situation that continues to this day.
For myself, I could not get my head around the idea that four implants were sufficient for a complete arch. With my extensive experience in placing implants, I thought I knew best. But Bo Rangert convinced me and a host of others that biomechanically it was sufficient, and in many ways, better for the patient.
While I was trying to decide what to do, the company was proceeding at a fast pace without me. The partners hired Dr. Mark Adams as lead prosthodontist. I thought this was a good start, as these types of treatments during the early 2000s were a work in progress, needing specialist expertise and ingenuity. In fact, there were three aspects to the treatment that had no significant scientific literature at that time, and these were:
- How to remove diseased teeth and prepare a clean foundation of bone for implants while at the same time obtaining enough interpositional space for prosthetic restoration.
- How to simultaneously treat both arches surgically and prosthetically. This had never been done before.
- How to get consistent immediate function in the maxilla, particularly an atrophic maxilla.
These extremely difficult clinical problems were solved over time and are now reported in the literature.4-8
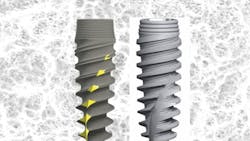
I was also tasked with deciding which commercial implant system to use, and it was a difficult decision. Dr. Ophir Fromovich visited from Israel and told me about a new implant (NobelActive, Nobel BioCare), which had both an aggressive thread pattern for primary stability and a curiously constricted neck for cervical bone preservation (figure 1). I found this to be an ingenious combination, something that intrigues me to this day as I now commercially sell an implant system that stands on the shoulders of this earlier innovation (Ultimate Implant, Ditron Dental).9,10
One day we sat around and debated the name for the company. Steve Boyd liked the words clear and choice and combined them together. The name ClearChoice remains to this day the leading brand.
The economic challenges
The difficult economic problems we faced in forming a clinic system for implant dentistry was something that had never been done before at scale.
There were three major problems:
- How to get eligible patients to call a central call center to make an appointment for consultation with the doctor.
- How to get people to go forward with treatment.
- How to establish sound economics that made sense to both the patient and the business considering the high cost of patient acquisition.
The development of an advertising message proved daunting, and the call center response equally so. Deutsch tried numerous messages, but it was themes about the patients themselves that took hold—what could be done for them rather than promoting prominence of the doctor or new high technology.
It was widely believed that cost factors or financing or insurance programs would be the key to success, but this was much less important than the psychosocial, that is, a person’s sense of health and well-being, and sometimes even their sense of purpose or meaning. It turned out the secret was spiritual—helping others to overcome a life interrupted, a life suspended by insurmountable dental problems. Tapping into that suffering with positive images of transformation for prospective patients elicited a sense of wonder.11
It took time for Deutsch’s message to resonate, as many people remained hesitant, even skeptical. Strangely, the dental profession strongly opposed what we were doing and thought immediate loading impossible to accomplish. Dental school faculty, many who had never done a single complete-arch treatment themselves, criticized ClearChoice medicine. We decided to take academia head-on. We wrote scientific articles and openly published our results in peer-reviewed journals. In the process, we reported several scientific findings that had never been reported before.Today, the all-on-four is taught in every dental school in the nation.
Despite these headwinds, hundreds of calls came into the call center. Calls would come in at 3:00 a.m., someone finally getting their courage up. The voice they heard was that of our call center director, Meredith Hertach, respectful, kind, caring, and real. That is why patients came. We gave them hope.
The call center, now called the Care Connection Team, ran 24 hours a day, seven days a week, and had over 100 staff. These highly talented individuals established the initial empathy and understanding for individuals taking their first step in resolving desperate situations.
At the consultation appointment, highly skilled patient education coordinators were trained by Dr. Miloni himself. Eventually, consult communication detailed a multistep process to help new patients feel at ease and accepted. Miloni’s dictum was: Turn a stranger into a friend.
ClearChoice developed many methods to educate patients so they could make an informed decision. Now we see ClearChoice messaging every day in almost every form of media, a tribute to this marketing genius that continues to impact our society in a very positive way.
The complex economics of this process were addressed by Steve Boyd and Margaret McGuckin. They arranged for a standardized financial structure including doctor contracts, procurement, and patient financing assisted by financial and accounting officers Jeff Adams and John Walton.
Following surgery, definitive treatment was carried out by Dr. Adams, assisted by laboratory technician Scott Adams, and associate Dr. David Haney. Lead surgical assistant, Cindy Formanek, and lead prosthodontist assistant, Monique Stocic, proved invaluable each step of the way. The initial treatment team was replicated, leading to many other surgical-prosthetic teams scattered all over the United States.
It is true that the clinic system grew and was sold for 10 figures, but economics is not always just about money; a true economy helps people. In the case of ClearChoice, hundreds of dentists, surgical and prosthetic assistants, and laboratory and management personnel gained employment. And approximately 150,000 patients suffering from debilitating and sometimes catastrophic dental conditions that hindered social interaction and employment opportunity have been aided in fulfilling their dreams.
Kevin Mosher summarized the impact of ClearChoice to patients and the dental profession: “The unique ClearChoice approach proved to be as powerful to practice economics as it did to efficient, predictable care. All nonclinical functions were handled by the central management company that, by spreading its costs over a large and growing network, was able to hire subject matter expertise in areas such as advertising and marketing, legal-regulatory, real estate, finance, and call center operations, which the sole practitioner could never economically justify.
The payoff is seen in the numbers. On an annual basis, the average ClearChoice clinic collects 7 to 10 times what the average private specialty practice collects, doctors earn 2 to 2.5 times more, and patient fees are generally 20 to 30% lower! As a result, access to transformative treatment has soared for patients with terminal dentition.”
Perhaps there is no single dental enterprise as significant to the dental profession as the ClearChoice initiative begun by Miloni and Boyd, which was serendipitously sparked by a Dental Economics magazine cover story more than 20 years ago.
Author's note: The author wishes to thank Gretchen Hale, ClearChoice executive assistant, for her valuable assistance.
References
- Schnitman PA, Wöhrle PS, Rubenstein JE, et al. Ten-year results for Brånemark implants immediately loaded with fixed protheses at implant placement. J Oral Maxillofac Implants. 1997;12(4):495-503.
- Dental Economics. 2001.
- Maló P, Rangert B, Nobre M. All-on-four immediate function concept with Brånemark system implants for completely edentulous mandibles: a retrospective clinical study. Clin Implant Dent Relat Res. 2003;5 Suppl 1:2-9.
- Jensen OT, Adams MW, Cottam JR, et al. The all-on-four shelf: mandible. J Oral Maxillofac Surg. 2011;69(1):175-181.
- Jensen OT, Adams MW, Cottam JR, et al. The all-on-four shelf: maxilla. J Oral Maxillofac Surg. 2010;68(10):2520-2527.
- Jensen OT, Adams MW. The maxillary M-4: a technical and biomechanical note for all-on-4 management of severe maxillary atrophy—report of 3 cases. J Oral Maxillofac Surg. 2009;67(8):1739-1744.
- Butura CC, Galindo DF, Jensen OT. Mandibular all-on-four therapy using angled implants: a three-year clinical study of 857 implants in 219 jaws. Dent Clin North Am. 2011;55(4):795-811.
- Graves S, Mahler BA, Javid B, et al. Maxillary all-on-four therapy using angled implants: a 16-month clinical study of 1110 implants in 276 jaws. Oral Maxillofac Surg Clin North Am. 2011;23(2):277-287.
- Danza M, Fromovich O, Guidi R, Carinci F. The clinical outcomes of 234 spiral family implants. J Contemp Dent Pract. 2009;10(5):E049-E056.
- Danza M, Riccardo G, Carinci F. Bone platform switching: a retrospective study on the slope of reverse conical neck. Quintessence Int. 2010;41(1):35-40.
- Klima RJ, Wittemann JK, McIver JE. Body image self-concept and the orthodontic patient. Am J Orthod. 1979;75(5):507-516
About the Author
Ole Jensen, DDS, MS
Ole Jensen, DDS, MS, received his DDS degree from Northwestern University School of Dentistry, and completed his anesthesiology residency at Northwestern University School of Medicine, and his oral and maxillofacial surgery residency at the University of Michigan. He is a Diplomate of the American Board of Oral and Maxillofacial Surgery and a Fellow of the American Dental Society of Anesthesiology. He lectures nationally and internationally, and has authored three textbooks on oral surgery and more than 25 articles.