Ask Dr. Christensen: Which dental technologies should I buy?
Q:
In every dental journal and at every dental meeting, I hear about new technology. Each company attempts to convince me that their technology is not only necessary for practice, but that it is the best in its category. I don't think I am much different than most dentists, and I don't have the financial resources to purchase many of these expensive items. Which technologies would you suggest for me, a typical general practitioner in a moderate-sized town with average US income?
A:
You are not alone. Most dentists are frustrated with the many new technologies that are currently on the market. Some of these technologies are immediately perceived to be valuable and become popular rapidly. Others are slow to be incorporated into practice and purchased by only some dentists. Many disregard these new technologies and continue to use conventional techniques.
I have some suggestions for you. To make decisions about what to purchase, you must carefully observe the characteristics of your own practice, your patients, your personal financial status, and the direction in which you want to grow your practice in the future. I will discuss various technologies and their advantages and limitations. It is interesting that the technology area of most change right now is oral and maxillofacial radiology.
I will identify the technologies I believe all dentists should consider obtaining as soon as possible, and also those that are highly useful for only some dentists where these specialized technologies fit their practice needs and desires.
Digital panoramic imaging
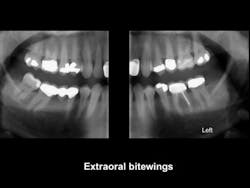
Currently, many dentists do not have digital panoramic devices. I suggest that this technology is one of the most important investments that you can make. Numerous brands are available. Look at them carefully, and purchase the brand that best fits your practice needs. Make sure that the device you purchase can be upgraded when you desire to incorporate cone beam or extraoral bitewing radiology into your practice (figure 1).
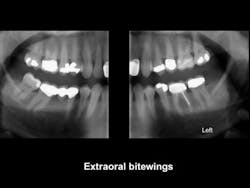
Figure 1: Extraoral bitewings provide excellent screening images of the maxillary and mandibular arches from third molar to lateral incisor with minimal overlap. They are available as an addition to most digital panoramic devices.
Digital radiographs, periapical and bitewing
Most dentists have already integrated this technology into their practices. The advantages are very clear, and they include ease of use; no messy developing and fixing solutions; ability to store the images and send them to other dentists or third-party payment companies; the ability to enlarge, colorize, and change images; low radiation; and others. The disadvantages include the high cost of sensors; thick, nonbendable CMOS sensors; frequent repair or replacement of some sensor brands; and inadequacy in identification of initial carious lesions.
Nevertheless, this technology is well recognized as an extremely valuable addition to a typical practice. Is any digital periapical or bitewing technology the same or better than CMOS sensors as described above?
Phosphor plate periapical and bitewing digital radiographs have some advantages when compared with CMOS sensors. They are far less expensive than CMOS sensors, they are thin and flexible, they create images equal to CMOS sensors, and they are easy to use. However, they do not make an immediate image and must be placed in a processor to transfer the images to a monitor.
Either CMOS or phosphor plate sensors should be in your office now. Also, if you have CMOS now, consider augmenting your radiographic procedures with the much less expensive but effective phosphor plate technology when you do not need an immediate image.
Cone beam radiology (CBCT)
This technology has been available for more than a decade, and I wrote about it in the Dental Economics March 2016 issue. Do you perform procedures in one or more of these areas: (1) implant placement, (2) removal of impacted teeth, and/or (3) endodontics? If so, you already at least need to have access to cone beam as this technology is rapidly becoming the standard of care.
The procedures in these three clinical areas are commonly accomplished in many general practices, and cone beam provides significant advantages over conventional radiography.
I suggest finding access to cone beam by one of the following methods:
• Buy a device if you have about $100,000 to spend.
• Join with a few other practitioners in close proximity to you and buy a cone beam device together. Put the cone beam device in a central clinical office, and find a radiographic technician to run and administer the device. Schedule days for each practitioner.
• Use a mobile cone beam company and have them come to your office routinely on specific days.
• Locate a radiographic clinic in your area and contract with them to make images for you.
You will need to take a course to learn how to read the cone beam images. You may not need cone beam immediately, but I strongly advise that you learn about it, find access to this technology, and save your financial resources to purchase a cone beam device in the future because this technology will soon be standard of care.
Technologies to consider, both new and old
The following are a few of the technologies that need your strong consideration because of their useful characteristics not available with conventional techniques.
Air polisher
This is an old technology. Some dentists have an air polisher, but most don't. I suggest that all general dentists should have an air polisher such as the Dentsply Cavitron Jet Plus, KaVo Prophyflex 3, or several others. As you know, these devices produce a slurry of sodium bicarbonate used to clean the enamel tooth surfaces of plaque and stain. Auxiliaries can legally use air polishers, which completely remove plaque. Why do about 50% of sealants come off within five years? Plaque is left in the grooves on the tooth being sealed. Can phosphoric acid etch remove plaque? Obviously not! The air polisher removes the plaque in the grooves, and the sealants cannot come out of the teeth.
Another relatively unknown use is detection of Class I caries. If a groovy tooth is cleaned with an air polisher and pigmentation still remains on the occlusal surface of the tooth, the likelihood of the tooth being carious in the pigmented area is very high. The pigment is still there after air polishing because it is under the enamel in a cavitated portion of the groovy surface.
You need an air polisher for the preceding two procedures plus numerous others.
Diode laser and electrosurgery
Cutting soft tissue or stopping blood seepage while preparing to make an indirect restoration impression is assisted by use of a diode laser or electrosurgery. If you are using the devices around any metal, laser is better because it does not cause sparks and heat. If you are just cutting soft tissue, electrosurgery is significantly faster, but it causes heat.
These devices are affordable, and I suggest that both should be in most offices for their different uses. There are many more expensive devices that you may also consider. Some examples of relatively inexpensive, proven devices are: (1) Parkell Sensimatic 700SE Electrosurge, (2) Biolase Technology iLase, and (3) Dentsply AMD Picasso Lite Diode Laser (figure 2).

Figure 2: Both electrosurgery units and diode lasers provide the ability to reduce or eliminate bleeding when doing soft-tissue management for impressions. Laser is better around metal because it emits less heat and doesn't cause sparking. Electrosurgery provides much faster cutting when removing a piece of soft tissue.
Elective but very useful devices
The following technologies are those that only some dentists have incorporated into practice, but those who have incorporated them have found them to be very valuable. I will list them with at least one of their major uses. Google them for specific information. All have been evaluated and found to fulfill their claims by Clinicians Report Foundation.
Air or hydroabrasion-Dentists can cut preps on patients without anesthetic or the noise of the screaming air rotor (PrepStart, Danville Materials).
Caries detection-Augment your ability to identify initial caries (CariVu, DEXIS; Microlux Transilluminator, AdDent; SoproCare, Acteon; CamX Spectra, Air Techniques).
Cancer detection-Screen for oral cancer on a routine basis (Bio/Screen, AdDent; DOE SE, DentLight; VELscope VX, DenMat; OralCDx, OralCDx Laboratories; ViziLite TBlue, DenMat; Identafi, DentalEZ).
Digital scanner-Replace your vinyl or polyether impression material with scanning. This technology is coming on very fast (3M True Definition Scanner, 3M; CS 3500, Carestream; CEREC Omnicam, Sirona; Planmeca FIT, Planmeca; iTero Element, Align Technologies; Trios, 3Shape).
Electric handpiece-Make a complete tooth preparation or just refine your preps. Experience high torque you have not seen before for cutting dentures, splints, or stone. These are the most used primary cutting instruments in many developed countries (KaVo, NSK).
In-office milling of restorations-Prepare and seat restorations in one appointment (CEREC, Sirona; Planmeca FIT, Planmeca; TS150, IOS Technologies).
Magnification-Enhance and improve your endodontic and some restorative procedures. These are standard of care in the endodontic specialty community (Global, Zeiss; MagnaVu PSII).
Monitors in your operatories-Many dentists now have two monitors in every operatory, one directly in front of the patient for radiographic images, patient education, and patient entertainment, and the other in the back of the operatory for recording details of the procedures, including financial information to be sent to the front office.
Occlusion-This technology, now refined and accepted for many nondental uses, scientifically locates occlusal contacts (T-Scan, Tekscan).
Surgical handpiece-You are probably removing impacted third molars and occasionally other impacted teeth, and you are considering placing implants, but you may not have a surgical handpiece, which allows lubricant during cutting and torque control (W&H; Aseptico).
Summary
There are many technologies available for dentists. Some of them are well accepted and used, and they are not included in this discussion. Other useful technologies should be in most practices but are not yet in many practices.
Technology is here! Look over the marketplace and incorporate those technologies that fit your practice and your financial situation.
Gordon J. Christensen, DDS, MSD, PhD, is a practicing prosthodontist in Provo, Utah. He is the founder and director of Practical Clinical Courses, an international continuing-education organization initiated in 1981 for dental professionals. Dr. Christensen is a cofounder (with his wife, Dr. Rella Christensen) and CEO of Clinicians Report (formerly Clinical Research Associates).