Taking a bite into sleep apnea

Arvin Ahmadieh, DDS
It’s scary to think about how many patients walk into our practices who have undiagnosed and untreated sleep apnea. A Frost & Sullivan report commissioned by the American Academy of Sleep Medicine estimates that 29.4 million Americans, or 12% of the US adult population, suffer from obstructive sleep apnea (OSA).1 Approximately 5.9 million adults are diagnosed with OSA in the US, indicating that 80% of the OSA cases remain undiagnosed.1 Frost & Sullivan further estimates that the associated costs of undiagnosed OSA amounted to $149.6 billion in 2015.1
As dentistry evolves into a more comprehensive field, it is our responsibility as dentists to include sleep apnea as part of our medical screening process. Oftentimes, we are the first clinicians who can perform screening and detect sleep apnea. Many patients visit their dentists more frequently than their physicians, and we must enhance our ability to provide comprehensive care for them rather than focusing solely on their teeth.
There are three steps dentists can take to identify and treat sleep apnea: conducting a thorough patient health history assessment, enhancing the patient exam, and offering oral appliance therapy.

Conducting a thorough patient health history assessment
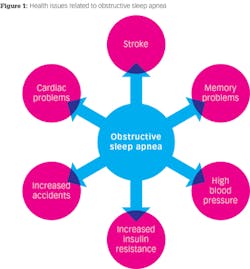
Obstructive sleep apnea is when an individual struggles to breathe or even stops breathing during sleep. OSA causes intermittent hypoxemia, sleep fragmentation, and stress on the heart, which can lead to health risks such as hypertension, cardiovascular disease, an enlarged heart, stroke, and more (figure 1).
Fortunately, dentistry is evolving and we’re taking much more into consideration when we collect patients’ medical histories. This enables us to screen for various medical conditions, including sleep apnea. It is easy to add questions to medical history forms to start the screening process for OSA. After reviewing a patient’s responses, we can follow up with questions such as:
- Do you snore in your sleep?
- When you wake up in the morning, do you still feel tired?
- Are you sleepy during the day?
- Do you wake up throughout the night?
The most telling sign of OSA is snoring. Loud snoring is caused by the tongue falling back into the airway and crowding with the uvula and soft palate. This crowding causes vibration of the tissue as patients breathe, and the vibration is heard as snoring. However, it’s important to note that just because someone snores doesn’t necessarily mean the person has OSA.
Once you start this conversation with a patient, follow up with the STOP-Bang Sleep Apnea questionnaire or the Epworth Sleepiness Scale to grade the person’s risk of OSA.2,3
Enhancing the patient exam
Based on the responses to these questions, a clinical evaluation can be conducted to screen for sleep apnea during the standard dental examination. Risk factors to look for include narrow patency of the airway, large tongue, large uvula, enlarged tonsillar tissue, large neck circumference, and elevated blood pressure.
If the signs and symptoms suggest that a patient may be suffering from sleep apnea, it’s appropriate to refer the person to a board-certified sleep specialist. A diagnosis is ultimately made with polysomnography, which is conducted in a sleep study facility. From there, the patient’s physician will classify the condition as mild, moderate, or severe OSA based on the number of times per hour the patient completely or partially stops breathing.
Possible treatment recommendations include weight loss, continuous positive airway pressure (CPAP), oral appliance therapy, surgery, or a combination of these.
Offering oral appliance therapy
The CPAP is the gold standard for treating sleep apnea without surgery.4 However, there are instances where patients cannot tolerate the CPAP and request an alternative option. This is where we can step in and aid in treatment.
Dentists can become involved with the treatment of OSA by creating an oral appliance. They are particularly effective in patients with mild to moderate OSA, and they function by moving the lower jaw forward, which subsequently moves the tongue forward to open the airway. The initial visit for the oral appliance is easy. Take upper and lower full arch impressions with polyvinyl siloxane, as well as a bite registration in centric relation. Then a lab will fabricate the device.
It is extremely important to review detailed instructions with a patient when delivering an oral appliance. It is also imperative to have very close follow-up with the patient during the next four weeks. The most common complications with sleep apnea oral appliances are symptoms of TMD. If you can titrate the protrusion of the jaw very slowly during the first few weeks, you can significantly reduce any discomfort. From there, follow-up can be done at the patient’s biannual dental exams.
It’s exciting that sleep apnea is another medical condition that dental professionals can screen for and help treat. By taking these three simple steps to conduct a thorough patient health history assessment, enhance the patient exam, and offer oral appliance therapy where indicated, we can help reduce the incidence of underdiagnosed and undertreated OSA. Working together, dentists and physicians can fight the ramifications of sleep apnea to improve the health of our patients.
References
1. Frost & Sullivan. Hidden health crisis costing America billions: Underdiagnosing and undertreating obstructive sleep apnea draining healthcare system. https://aasm.org/resources/pdf/sleep-apnea-economic-crisis.pdf. Published 2016. Accessed March 26, 2018.
2. Chung F, Subramanyam R, Liao P, Sasaki E, Shapiro C, Sun Y. High STOP-Bang score indicates a high probability of obstructive sleep apnea. Br J Anaesth. 2012;108(5):768-775.
3. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-550.
4. Spicuzza L, Caruso D, Di Maria G. Obstructive sleep apnea syndrome and its management. Ther Adv Chronic Dis. 2015;6(5):273-285.