Resin-modified glass ionomer: The open sandwich technique

Dr. Ian Shuman discusses one of the uses for the new resin-modified glass ionomers as a base for Class II and III direct composite restorations, known as the "sandwich technique."
In 1972, Wilson and Kent introduced glass ionomer cements that cured via a simple acid-base reaction. (1) When the two components (glass and acid) were mixed, these materials "self-cured." Twenty years later, "resin-modified glass ionomer cements were developed that could be light-cured." (2) The term "resin-modified" denotes the addition of resin groups (i.e., HEMA) by virtue of the attachment of these molecular groups to the "acidic liquid component." (3) These light-cured, resin-modified glass ionomer (RMGI) cements offered many benefits. The speed of light-curing vastly shortened the setting time that had been a significant shortcoming of the original self-cure glass ionomers. In addition, the release of fluoride ions was thought to challenge recurrent caries from developing.
The New RMGIs
Most recently, a new group of light-cured RMGIs has been introduced, all with varying recommendations and abilities (e.g., Ionolux, Voco; GC Fuji II LC, GC America; Photac Fil Quick Aplicap, 3M; Riva Light Cure, SDI). One material, Ionolux, has demonstrated a wider variety of applications than previously recommended for RMGI materials. This modified restorative does dual-cure in that the glass ionomer aspect self-cures with an acid-base reaction and the resin aspect is light-cured, similar to other RMGI brands on the market. It has composite-like esthetics, nonsticky handling, and is immediately packable. This material offers enhanced physical properties, continued fluoride release (found in original glass ionomers), better longevity, does not require dentin conditioning, and is excellent at preventing leakage from intraoral fluids with a low water solubility coefficient, thus preventing fluid absorption (tables 1 and 2). One of the uses of these RMGI materials has been as a base for Class II and III direct composite restorations, known as the "sandwich technique."

The sandwich technique
When a carious lesion and the Class II cavity preparation extend near to or apical to the cementoenamel junction, the sandwich technique can be used. The technique is described as a layering of various restorative materials within the cavity preparation. It involves placing RMGI at the base of the cavity preparation, followed by curing and the addition of composite restoratives to complete the restoration. If the remaining layers of composite resin completely encase the RMGI, it is considered a "closed" sandwich technique. If the RMGI is exposed to the oral environment at the base of the restoration, it is considered an "open" sandwich technique (figures 1a and 1b).
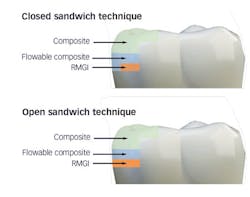
Figures 1a and 1b: RMGI sandwich techniques
This technique is not new and was originally proposed by Suzuki and Jordan. (4) According to Liebenberg, "The open-sandwich technique allows the least amount of microleakage of the various direct restorative options currently available." (5,6) This occurs because traditional composite bonding at the cavosurface and interproximal sites often have a complex combination of substrates that include enamel and varying levels of dentin, depending on the depth of the lesion. Liebenberg continues, "For dentin bonding, it appears far easier to achieve a seal than to maintain it, and in vivo studies have confirmed that resin-dentin bonds degrade in the oral cavity." (5,7)
Clinical technique
The patient, a 29-year-old man, presented with a failing Class II direct composite restoration in the upper left second premolar (figure 2). A radiograph confirmed the presence of a carious lesion (figure 3). Due to the recurrent caries found in many of the teeth, a conservative treatment plan was made for possible root canal therapy and a direct composite restoration. In cases with recurrent caries, using an RMGI is ideal in that it contains fluoride and provides a more suitable "environment" for restoring deep lesions.

Figure 2: A failing Class II direct composite restoration in the upper left second premolar

Figure 3: Radiograph confirming carious lesion

Figure 4: Preparation after restoration removal

Figure 5: Triodent (Ultradent) sectional matrix system in use
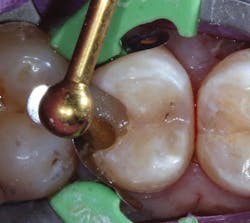
Figure 6: Application of Ionolux as a base layer

Figure 7: Light-curing of Ionolux

Figure 8: Ionolux after light-curing

Figure 9: Application of Futurabond U

Figure 10: Application of Admira Fusion in process

Figure 11: Preparation after completed application of Admira Fusion

Figure 12: Final radiograph of restoration
The tooth was anesthetized using 4% articaine with 1:200,000 epinephrine x 1.8 cc. The upper left posterior quadrant was isolated using a rubber dam. Following removal of the restoration (figure 4), gross caries was removed using a #6 round stainless steel slow-speed carbide followed by #6 and #4 round slow-speed polymer SmartBurs II (SS White). Complete caries removal was determined by explorer examination and evaluating the existence of cariogenic bacteria using fluorescence (Spectra, Air Techniques). A Triodent sectional matrix system (Ultradent) was placed (figure 5), followed by the application of a base layer using Ionolux RMGI (figure 6). In addition, the Ionolux RMGI was selected for this case due to its high compressive strength, approaching levels seen with the newest generation of flowable composite resins. (8,9) The Ionolux was compressed into the preparation in what was the initial layer of the open sandwich technique. Following the light-curing of the Ionolux (figures 7 and 8), Futurabond U (Voco), a dual-cure universal adhesive in a single-dose delivery system, was applied to the preparation and light-cured (figure 9). Admira Fusion (Voco), a universal light-cured, nanohybrid, organically modified ceramic (ORMOCER), was placed in 2-mm increments. Each increment was light-cured until the restoration was completed (figures 10 and 11). A radiograph was taken to evaluate the immediate success of the restoration (figure 12). The Ionolux RMGI demonstrated excellent opacity, comparable to composite resins.
Summary
Resin-modified glass ionomers have been used for more than 20 years and have provided numerous benefits to dentistry. With the newest class of RMGIs, additional areas of use have provided new applications for this material, benefitting patients and clinicians alike.
Ian Shuman, DDS, MAGD, AFAAID, maintains a full-time general, reconstructive, and esthetic dental practice in Pasadena, Maryland. Since 1995 Dr. Shuman has lectured and published on advanced, minimally invasive techniques. He has taught these procedures to thousands of dentists and developed many of the methods. Dr. Shuman has published numerous articles on topics including adhesive resin dentistry, minimally invasive restorative dentistry, cosmetic dentistry, and implant dentistry. He is a master of the Academy of General Dentistry, an associate fellow of the American Academy of Implant Dentistry, and a fellow of the Pierre Fauchard Academy.
References
1. Wilson AD, Kent BE. New translucent cement for dentistry. The glass ionomer cement. Br Dent J. 1972;132(4):133-135.
2. Frankenberger R, Sindel J, Kramer N. Viscous glass-ionomer cements: a new alternative to amalgam in the primary dentition? Quintessence Int. 1997;28(10):667-676.
3. Hewlett ER, Mount GJ. Glass ionomers in contemporary restorative dentistry-a clinical update. J Calif Dent Assoc. 2003;31(6):438-492.
4. Suzuki M, Jordan RE. Glass ionomer-composite sandwich technique. J Am Dent Assoc. 1990;120(1):55-57.
5. Liebenberg W. Return to the resin-modified glass-ionomer cement sandwich technique. J Can Dent Assoc. 2005;71(10):743-747.
6. Loguercio AD, Alessandra R, Mazzocco KC, et al. Microleakage in class II composite resin restorations: total bonding and open sandwich technique. J Adhes Dent. 2002;4(2):137-144.
7. Hashimoto M, Ohno H, Kaga M, Endo K, Sano H, Oguchi H. In vivo degradation of resin-dentin bonds in humans over 1 to 3 years. J Dent Res. 2000;79(6):1385-1391.
8. Filtek Supreme Ultra Flowable Restorative technical product profile. 3M website. http://multimedia.3m.com/mws/media/677816O/filtek-supreme-ultra-flowable-technical-product-profile.pdf. Accessed December 22, 2016.
9. Hegde MN, Hegde P, Bhandary S, Deepika K. An evaluation of compressive strength of newer nanocomposite: An in vitro study. J Conserv Dent. 2011;14(1):36-39. doi:10.4103/0972-0707.80734.