Increasing efficiency and productivity in general dentistry

By Guy Gross, DDS
Contemporary dental offices are evolving to perform "super" dentistry. The dictionary defines "super" as "above and beyond."By offering patients expanded options, we go above and beyond the usual scope of general dentistry, striving toward our goals of clinical excellence while keeping patients in-house and increasing productivity.

At New Horizons Dental Care in Salina, Kansas, as a group practice of GPs, we use cone beam 3-D imaging to help us reach our goals with increased precision and confidence. In our practice, each doctor has a unique skill set and we all work as a team to care for patients. I focus on implants, surgical treatments, and cosmetic dentistry. My wife, Dr. Kate Gross, offers all forms of orthodontic treatments. Dr. Allison Lesko treats many of our pediatric patients, performs IV sedation, and enjoys hard and soft tissue grafting cases.
Here are just a few of the areas in which our cone beam system has helped us expand our capabilities:
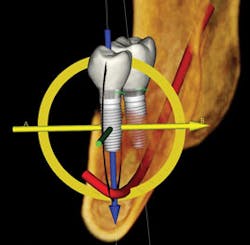
For implants -- 3-D imaging gives us total confidence by offering a thorough analysis of bone structure, bone volume, and tooth orientation. With Tx STUDIO™ software that is exclusive to the i-CAT® brand, I can see if the implant can be placed in its optimal position or if the site needs a graft first. This results in optimized diagnosis and treatment planning tools so that a realistic and understandable treatment plan can be presented to the patient. I often plan the implants alongside the patient.
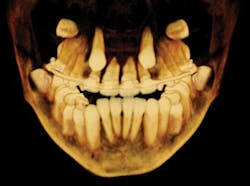
For orthodontics -- 3-D imaging has allowed our practice to expand the orthodontic procedures that we offer. We treat Class I and Class II cases in-house, with applications such as traditional banding, Invisalign®, and Six Month Smiles. To help plan for optimal orthodontic treatment, the scan shows us root angulations that may be problematic from the start, supernumerary teeth, and other anatomical landmarks. Our cephalometric analyses are now plotted very precisely in space due to the ability to rotate the image and "go inside" the skull. We can compile images into a virtual study model that shows roots, developing teeth, impactions, and alveolar bone. These can be shared with orthodontists to whom we refer our Class III skeletal discrepancies.
For TMD and surgical cases -- A cone beam scan helps us assess the joint health and risk management prior to complex reconstructive cases, and helps in precise positioning of wisdom teeth so that we know whether to treat or refer patients to an appropriate specialist.
For endodontics -- Before starting endodontic treatment, we can use the scan to determine the number of roots and canals, whether there are any "crazy" curvatures of those canals, and of course, apical lesions, which are often obscured by the maxillary sinus. We can look at the canals from every possible viewpoint. In diagnosing root fractures, we can see the details of the area, such as bone loss or perforations from previously placed posts. This precise view makes a huge difference in terms of our efficiency and predictability of the cases we're starting. It also makes our schedule much more predictable.
For dental sleep medicine -- When we work with sleep physicians and prepare to fabricate sleep appliances, we use 3-D scans along with other criteria for screening and diagnostic purposes. For airway assessments, we can see restricted airways and calculate detailed measurements. Our 3-D data can be shared with the sleep treatment team. I've found that it is not a stand-alone diagnostic for OSA, but an excellent screening tool that facilitates great discussion with patients.
Another big plus is that we can capture these highly detailed scans with minimal radiation exposure to patients. My office has an i-CAT Next Generation, which has the option to produce 4.8-second scans and a variety of scan sizes with a lower dose to patients. We get low amounts of radiation and tremendous amounts of information.
We did not acquire the cone beam in order to increase production through scans. We saw it as a no-brainer for doing better dentistry because of the information We gained from the scans. Increased production has been a nice result. While we do not necessarily strive to make a profit on the scans themselves, the increased amount of detailed information definitely leads to more succinct diagnosis, better treatment planning, more case acceptance, increased patient education, and better compliance. When I do work with referring dentists or specialists, I can easily and securely email scans to their offices. It is one of the most productive pieces of equipment in my office, from diagnosis to treatment implementation.
Dr. Gross is not employed by Imaging Sciences. He does not act as a consultant for them, nor does he have any financial interests in the company.
Guy W. Gross, DDS, graduated with honors from the University of Missouri-Kansas City School of Dentistry. He has dedicated himself to advanced training in areas such as cosmetic dentistry, endodontics, implantology, occlusion, periodontics, and business management.
Past DE Issues