Commit to saving lives through early oral cancer detection
by Jonathan A. Bregman, DDS, FAGD
For more on this topic, go to www.dentaleconomics.com and search using the following key words: oral cancer, oral cancer detection, cancer exam, cancer test, Dr. Jonathan Bregman.
Although I have read and spoken these statistics numerous times, these negative statistics still shock me.
Every hour, of every day, of every month, of every year someone dies as a result of oral cancer.
- The five–year survival rate of 50% for oral cancer has not changed in the past 35+ years.
- Of all the new cases of oral cancer diagnosed this year, 25% of those occur in individuals who do not have the previously accepted standard risk factors for the disease, with a significant percent having no known risk factors.
- HPV 16/18 infection has a direct correlation to oral cancer through sexual activity with the population of concern 18 years (some say 13 years) and older. The increase of oral cancer in this younger population has increased sharply in recent years.
- In a recent nationwide survey, the percentage of patients that reported receiving a complete oral cancer examination at their last dental visit was 20%. One recent statewide survey showed 31%.
Thankfully, there are some positive statistics:
- Early detection and diagnosis of oral cancer can improve the five–year survival rate to 85% to 90%.
- As with mammography for breast cancer, colonoscopy for colon cancer, and PSA for prostate cancer, new adjunctive technologies to the complete oral examination can dramatically improve early detection of oral cancer. Untold numbers of lives can be saved.
- The Garasil vaccine (by Merck, Inc.), a series of three injections (especially when received prior to the onset of sexual activity), will not only dramatically reduce the rate of cervical cancer caused by HPV, but will reduce the related rate of oral cancer as well.
The key to improving negative statistics
So the key to improving all of the negative statistics revolves around two key issues:
- Complete oral examination (COE)
- Adjunctive technologies
Moving the dental profession more consistently in this direction will not only save lives and build practices, but reduce the growing number of lawsuits related to oral cancer detection.
A word about human papillomavirus (HPV 16/18)
The standard age range to do an early oral cancer screening has changed from 40 to 18 (or 13) and older due to the alarming rise in the incidence of HPV 16/18. Most people know that this virus, with its many subtypes (thus the numbers) are proven to contribute to cervical cancer. What many do not know is the direct correlation between HPV 16/18 and oral cancer that is spread through sexual activities to the mouth. The increasing number of people in the 18 to 40 age range with diagnosed oral cancer is startling. In my opinion, the entire dental profession has to change direction and begin comprehensive screening, medical/social history review, and counseling of individuals beginning as early as age 12 regarding the fatal sequella of becoming infected with the HPV virus. It is becoming an epidemic.
Components of a complete examination
Very clearly stated, the earlier the diagnosis, the higher the survival rate. We were all taught the "how to" in dental, dental hygiene, or dental assisting school. It is a systematic examination of the extraoral and intraoral structures. It can be accomplished in a one–and–a–half to two–minute time frame. The examination is both visual (using incandescent or white light) and bimanual (using both hands). All findings, both negative and positive, must be recorded, because if left blank, medico–legally, they were not performed. Thorough, complete, and recorded are the three words that must be kept in mind. Period! We all know how to do this. It is our professional responsibility to provide this service to all of our patients.
Adjunctive technologies
Note that I have used the word "adjunctive." The reason is that all of the available technologies related to oral cancer detection are, indeed, "adjunctive." The complete oral examination (COE) must be performed first, then the technologies come into play to improve the likelihood that any abnormal lesions will be detected or discovered.
Note: Detection does not equal diagnosis. The only way a true "diagnosis" is made is by the "gold standard" of biopsy (incisional or excisional) obtained through scalpel or laser. The adjunctive technologies, then, help us to discover or more readily detect abnormalities in the oral cavity that we might have missed with the naked eye alone and white (incandescent) light.
Technologies 101
In the past six months, I did my "due diligence" research.
What has become clear to me is that, yes, there needs to be more clinically based research performed at multiple sites ...
- Using a general population, not an "at risk" population of patients.
- Performed by independent researchers who have absolutely no affiliation with any one manufacturer either financial or otherwise.
But, and here comes the but, there is a growing base of knowledge available to dental professionals now to make an informed decision and then use one or all of these technologies. Not one of the technologies is harmful in any way to a patient. They each can provide an opportunity to, at the least, enhance the discovery of abnormal lesions not seen with only white light. Let's stop arguing about what has value, learn what they can do for us, and move forward and save some lives.
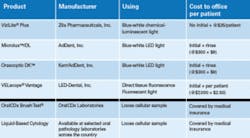
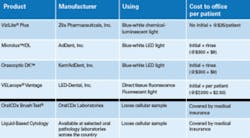
These are the products currently available for early oral abnormal lesion detection: ViziLite® Plus (Zila Pharmaceuticals, Inc.), Microlux™/DL (AdDent, Inc.), Orascoptic DK™ (Kerr/AdDent, Inc.), and VELscope® Vantage (LED–Dental, Inc.). For summaries of how to use the products, go to www.dentaleconomics.com and click on the Download Center.
A moral and ethical question we must ask
Personally, I feel that COE and any adjunctive technology used should be a part of the standard of care in all offices and performed on every patient when appropriate. If, for example, only 25% of your patient population "chooses" to have an adjunctive oral cancer screening due to additional fees for same, what about the other 75%? Is that the moral and ethical thing to do to restrict potentially life–saving care to only those who can afford or see value in an additional screening modality? Why does the use of these technologies need to be a money–making proposition for the office? Can't we just add a small amount to our examination fee to cover basic costs? I challenge you to think about this moral/ethical question and find your answer by leading with your head and your heart.
Your practice … your future
The ultimate purpose of all technologies in dentistry is to improve patient care. In the realm of early oral cancer detection, we now have adjunctive technologies to the COE that will dramatically aid dental practitioners. The earlier the "abnormality" is discovered and diagnosed, the better the survival rate for that individual.
There will be some who don't like my simplified conclusions. I defend myself in advance of these comments simply by saying that this is my overview of this topic and an effort to ...
- Encourage the most important action we of the dental profession can take: Do a complete oral examination on all patients beginning at age 18.
- Encourage dental professionals to use their own good judgment and choose either one or all of these technologies for their patients.
No one can refute the fact that we have to discover abnormalities earlier if we are to save lives. As the research becomes available, things will change; however, what will not change is the need for us to do more than we are doing right now. If what we do now is no different than what we did 35 to 40 years ago, we as a profession have failed the very people for whom we have been entrusted to care.
It is your practice. It is your future. Choose wisely the course that you will take.
Jonathan A. Bregman, DDS, FAGD, is a clinician, speaker, author, and trainer who led successful dental practices for more than 30 years. While dedicated to improving the dentist, team, and patient experience, he has a passion for educating dental professionals about early oral cancer detection and laser–assisted dentistry. You may contact Dr. Bregman by e–mail at [email protected] or visit www.bregmandentistry.com.