Outcomes-based practice — Part 3
by David W. Chambers, EdM, MBA, PhD
How outcomes-based practices get better
Outcomes in dentistry are different from those in other areas. Dental outcomes are particular, personal, and practical.
Practicing dentistry is not the same thing as repeating dental procedures. In fact, some dentists have done the same procedures over and over again for years and have complied with state-mandated CE requirements, but they haven't practiced more than a day or two in their lives. The result of repetition without practice is boredom.
Practice requires cycles of repetition with the brain turned on. In particular, a practitioner must be acutely and simultaneously aware of three things: why the activity is being done, how it feels to do the activity, and what the outcomes are. Learning in practice means being aware and responding.
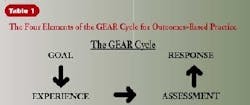
Different levels of learning are possible in practice, depending on whether dentists pay attention to anything in the process and what they pay attention to. Four stages are always involved in dental procedures, in overall practice, and in dentists' personal lives - Goals, Experiences, Assessment, and Response. Together these elements form a loop called the GEAR cycle. (See Table 1.) Mindlessly cycling through these stages leads to endless repetitions, like a car in neutral. Racing the engine won't help much.

The difference between meaningful behavior and random or reactive acts is the presence of a goal. Goals are double-vision images of the current condition and what is possible. They aren't a mission statement - don't confuse a statement with a mission. Goals are pictures so clear they can be described to others and used as a template to compare the difference between what is and what ought to be. Such sharply focused disparity creates motivation.
Much of what happens in continuing-education courses is goal-setting. Few CE courses change dental practice directly. For the most part, they show what is possible. Those dentists who alter their goals later learn how to achieve them in their own offices.
Experience is the activity intended to achieve the goal. The word "experience" is used rather than "activity," in order to emphasize awareness in action. Experience is the difference in sensation between cutting enamel and dentin, the sound of your own voice during treatment presentation, and awareness of the change in your posture as the day progresses.
Experience also must be connected with a goal or it is no more than random behavior. Experiments of this type have been conducted frequently, but one of the oldest was a study at MIT. In the experiment, two cats were connected by a series of harnesses and levers so that the activities of one cat were duplicated exactly by the second. The first cat - the one acting on its own and with purpose - was put through a series of learning trials, while the second cat passively engaged in the same activities. On subsequent testing, the first cat demonstrated learning while the second did not. Participation without purpose is not practice.
The third element in continuous improvement is assessment. Assessment means looking at the results of experience relative to goals. Is the marginal shrinkage on this new material within tolerable limits? Does the new way of scheduling patients produce fewer gaps on the book? Assessment is more than measuring whatever is convenient. It must connect the goal and the experience. Golfers don't improve their game simply by shooting a low score on a particular day. They learn by reflecting on how it feels when trying various alternatives. Or, as my great aunt used to say, "No one loses weight just because they buy new bathroom scales."
This threaded, triple sensitivity to what is intended, what is experienced, and what the results are is called an outcome. Outcomes go beyond objective results; they are simultaneous, intelligent, sensitive comparisons of goals, experiences, and assessments in practice. This is what outcomes-based practice is about.
There are four stages in the GEAR cycle for continuous improvement in practice. Achieving outcomes and being aware of what they are is not sufficient to improve practice. Outcomes must be used in some intelligent fashion. The fourth element in the GEAR cycle is response - what is done about outcomes. There are seven different responses possible, and the combination of responses dentists choose determines the level of learning possible in practice. In the next few articles, we will talk about reacting (Level 0 Learning), learning that focuses on reworking failures or rejecting them to improve overall practice performance (Quality Assurance or Level 1 Learning), and re sponses that promote continuous practice improvement by changing the goals (reconsideration), the experiences (redesign), and assessment (reassessment) (Level 2 Learning). The ultimate response is reflection - an integration of all learning in practice.
Outcomes are not the same in dentistry as in many other endeavors. There is a significant difference between a practice and a business, for example. Practices always make something. Often, this is something that can be held in one's hands, but it is always something that can be assessed against the two-part standard of functionality and esthetics. Dentists who are not asking on a constant basis whether their work functions as intended and is beautiful are not really practicing. They may be producing like heck, but I will wager dollars to doughnuts that they are frustrated and bored and that their practices have not improved in years. And they never will because continuous improvement demands a personal investment in beautiful things that work.
Outcomes in dentistry are different from those in insurance, .coms, or government. Some kinds of research meet the criteria of practice as well - true researchers discuss "building powerful and elegant theories." Those who conduct clinical trials for hire or test practices for evidence-based dentistry seldom talk this way. Dental outcomes are particular, personal, and practical. There is an inherent "yes!" quality about practice outcomes.