Success with Sedation: A Profitability Comparison of Nitrous, Oral, and IV Sedation
For more on this topic, go to www.dentaleconomics.com and search using the following key words: success with sedation dentistry, Dr. Anthony Feck, Dr. Michael Silverman, profitability comparison, oral and intravenous sedation, sedation modalities.
Introduction
Perhaps no other discipline in dentistry has enjoyed as much growth over the last decade as sedation dentistry. The use of oral (enteral) and intravenous (parenteral) sedation has evolved from a procedure provided primarily by specialists, to an accepted mainstream procedure practiced by more than 40% of U.S. general dentists.
When practiced according to industry standards by trained providers, sedation dentistry has proven to be a safe, effective tool to manage a wide range of patients, including those who suffer from dental anxiety, moderate to severe gaggers, people who want longer and more productive appointments, patients in need of complex restorative treatments, and those who have a resistance to local anesthetics.
Many dentists now realize another benefit of sedation dentistry: high profitability. This article will examine profitability by comparing three sedation modalities — nitrous oxide, oral, and intravenous.
The profitablity formula
Profitability can best be measured by evaluating key practice parameters through an equation called the profitability formula. This says that profit is the result of production multiplied by collection rate minus expenses. If we accept this, then we can compare nitrous oxide, oral, and intravenous sedation by examining the impact each has on these three components.
Production
Increased production is the most obvious benefit to the dental business when sedation dentistry is incorporated. Dentists who employ sedation enjoy more new patients and increased case acceptance, as well as higher production value per patient.
Sedation dentistry naturally caters to high–fear patients. Every dentist treats anxious patients daily who could benefit from being more comfortable. Many more patients aren't being treated at all due to anxiety. Offering this service has opened the door to hundreds of thousands of patients across the country who previously avoided dental care.
Since much of the dentistry completed on new patients occurs within their first year as patients, the influx of sedation patients will naturally result in more production. Also, many patients who would be referred to specialists for sedation can now be seen by the general dentist trained in these services.
On the surface it may seem counterintuitive that the sedation candidate would accept dentistry at a higher rate than the noncandidate. After all, these patients have two primary obstacles to case acceptance: fear, and the cost of an extensive treatment plan (often the result of years of neglect).
Many practices find that the dominant obstacle is fear. Once patients are assured they'll be comfortable, any financial roadblocks are overshadowed. The patient's desire to have a healthy, attractive smile and be free from pain or embarrassment takes priority.
The average sedation patient has extensive dental needs, which translates to higher overall production value potential to the practice per patient. The size of the treatment plan is often measured in tens of thousands of dollars. The nature of the sedation process typically results in longer appointments, so the doctor's schedule contains more productive appointments when compared to nonsedation care.
When sedation patients are comfortable and their needs are treated in fewer appointments, care is delivered more efficiently, which results in more dentistry being performed per unit of time.
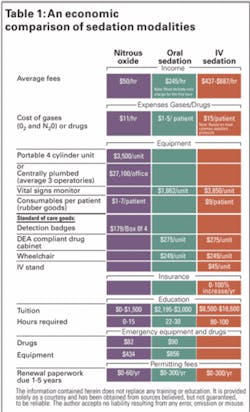
Additionally, there are added charges related to the delivery of the sedation itself. Depending on the type of sedation provided, the average fee for the sedation portion of the appointment can range anywhere from $50 for nitrous oxide, to $245 for oral sedation, and $562 for intravenous sedation, which makes the anesthesia portion of the procedure a profit center in and of itself (see Table 1 on page 32).
In general, due to its pharmacological characteristics, oral sedation allows for longer appointments than either nitrous oxide or intravenous methods. Therefore, it has the greatest potential for increased production.
It can be argued that intravenous sedation has as much, if not more potential than oral sedation due to its efficient delivery. It allows for more cases to be treated in less time. Regardless of this debate, nitrous oxide sedation finishes third in this comparison due to its shorter duration per appointment.
Collection rate
The collection rate is affected by the financial policies of the office, as well as any adjustments made by the difference between maximum allowable charges (from participation in a third party in–network plan), and the fees of the practice. All things considered, the collection rate for oral and IV sedation is greater than nitrous oxide due to most office policies requiring payment in advance of treatment.
The justification for such policies lies in the fact that large blocks of time are set aside for these long, productive appointments. Also, collecting money from a sedated patient at the time of the appointment has legal and ethical repercussions. Sedation with nitrous oxide alone, given its minimal level of sedation and its transient nature, does not necessarily require payment in advance of the appointment.
Therefore, it is not accompanied by the same collection rate benefits as oral and intravenous sedation. However, when it comes to third party allowances and insurance reimbursement, nitrous oxide sedation is much more likely to be a covered expense.
Expenses
As with any discipline of dentistry, there will be expenses related to its delivery, ranging from training for the doctor and team to supplies and equipment. In the case of sedation, certification and recertification expenses apply. Table 1 compares the expenses associated with nitrous oxide, oral, and intravenous sedation.
Regarding supplies, the cost of the anesthetic and associated medications for all three modalities is a fraction of the cost of administering sedation. However, nitrous oxide and oxygen gases are more expensive per appointment than either oral or intravenous drugs. Yet nitrous oxide sedation is fast, like intravenous. Both require only minutes to work. Oral sedation is the slowest, requiring 30 to 90 minutes for onset.
Equipment associated with each sedation method can be divided into that necessary for the delivery of the anesthesia, supportive equipment required by regulatory agencies, and equipment considered the standard of care.
The equipment required for each sedation method can be divided into start–up and ongoing expenses. Nitrous oxide is the most expensive, costing $3,500 per portable dispensing unit and about $27,100 to centrally plumb a facility for three operatories. While oral and IV sedation don't require facility changes, they do necessitate additional monitoring equipment.
The standard of care everywhere is to continuously monitor a sedation patient's heart rate, oxygen saturation, and blood pressure intermittently (for sedation above and beyond what is typically achieved with nitrous oxide).
Some state regulatory agencies also require this. IV sedation, with its potential for deeper levels of sedation, may require monitoring heart rhythm and expired carbon dioxide. Therefore, the costs for standard of care pulse oximetry plus additional monitors can range from $1,862 for oral sedation, to as much as $3,850 for IV sedation (see Table 1).
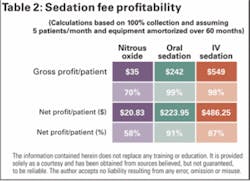
Having an automated external defibrillator (AED) on–site and pharmacology software to check for drug interactions is also considered the standard of care for all sedation methods. For oral and intravenous sedation, other supportive equipment (see Table 2 on page 33) is necessary for the secure storage of medications and the safe transport of the patient following sedation. With IV sedation there are additional consumables necessary for the administration of IV fluids.
The bottom line with equipment and sedation is that nitrous oxide has the greatest start–up costs if administered centrally, but much lower costs if it's administered using a portable unit. IV sedation requires the greatest start–up investment. With regard to ongoing expenses, IV sedation is the most expensive, and oral sedation is the least.
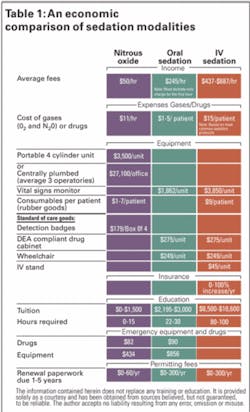
When it comes to education and permitting fees, intravenous sedation has the greatest expense, followed by oral sedation, and then nitrous oxide.
The sum of the expense comparison associated with these three forms of sedation shows that the highest overhead is associated with IV, followed by oral and nitrous oxide sedation. The average fees charged in dental practices for these services reflect these expenses.
Conclusion
In comparing the profitability of these three forms of sedation, we have looked at three factors: production, collection rate, and expenses. It must be understood that there is great individual variability with each of these disciplines, and as such there is no clear winner when it comes to profitability.
How the practitioner uses these methods has as much to do with the bottom line achieved as does the inherent potential that each has for profitability. To further complicate any comparison, many practitioners employ a combination of these forms of sedation.
It was determined that oral sedation had the greatest potential for production, while both oral and IV sedation typically do best with collection rate. In terms of expenses, there is a wide range of possibilities for start–up, ongoing, and educational costs.
Based on the above, and faced with choosing a winner for profitability, oral sedation carries the day. There is no question that sedation dentistry has been a boon to dentistry. The return on investment from implementing these services has rewarded many dentists with more enriching practices, both personally and professionally.
Although this article has focused on practice profitability, the clear winner has been and will continue to be patients, whose health and well–being are often transformed through sedation.
References available upon request.
Anthony Feck, DMD, DDOCS, is a nationally recognized clinician, consultant, lecturer, and author. He maintains a private practice in Lexington, Ky., that focues on oral and IV sedation. He is the dean of faculty for DOCS Education. Reach Dr. Feck at (866) 592–9613 or [email protected].
Michael D. Silverman, DMD, DDOCS, DICOI, is an internationally recognized dental educator, business leader, marketing expert, entrepreneur, speaker, and author. He is the cofounder and president of DOCS Education (DOCSeducation.org), which provides CE training, products, and membership to dentists and teams on sedation dentistry and emergency preparedness. Dr. Silverman can be reached at (866) 592–9613 or Dr.Silverman@DOCSeducation.