Narrow-diameter implants: Making impossibilities realities

Narrow-diameter implants: Making impossibilities realities
Adam Koppelman, DMD
Using social media to post photos is a relatively new occurrence. Facebook was founded in 2004. Instagram emerged in 2010. In 2013, the Oxford Dictionary added the term “selfie.” In the same year, “selfie” was named “word of the year.”1
Patients—both young and old alike—are more conscious of their smiles and the way they look. Teeth are front and center in the mouth-centric Snapchats and Instagrams sent and received every day. Patients are reminded of their smiles, and what they’d like to change about them, when they are tagged unexpectedly in photos. Today, we see more patients seeking dental treatment as a result of social media: grandmas noticing their smiles as they FaceTime with their grandkids, or the teen known for her “duck face” because she’s really trying to hide her smile.
No one wants to walk around with missing teeth or flippers that are uncomfortable, but it is incredible how many patients do because they have been told “You don’t have enough room for an implant,” or “You’ll need a grafting procedure before we can place an implant there.”
According to facts and figures from the American Academy of Implant Dentistry (AAID) and independent data from Millennium Research, of the patient population who actually goes to the dentist, only 10% of those who could benefit from an implant actually proceed with treatment.2,3 That’s a lot of business left on the table. The AAID also reports that the implant and prosthetic market is expected to reach $6.4 billion by 2018.3 With billions of dollars fueled by a mere 10% of the patient population, any one of us would be happy to capture even a fraction of this market as it grows.
By offering narrow-diameter implants in our practices, we’ve turned impossibilities into realities for our patients. We offer them something they’ve been told couldn’t be done. We offer them hope, and hope is pretty powerful. Not only have we seen an increase in our implant case acceptance, patients are so satisfied and grateful for the second chance they’ve been offered that our word-of-mouth referrals have become an incredible resource.
There are a lot of mistruths out there about narrow-diameter implants, also referred to as small-diameter implants (SDIs) or mini-implants. As Gordon Christensen, DDS, states, “The truth is diametrically opposed to what some are saying, and it has been our observation that some of the most severely negative comments come from dentists who have never placed SDIs.”4
The research is there. Just this month, Stuart Froum, DDS, and the implant team at New York University published an impressive 14-year follow-up on narrow-diameter implants, evaluating peri-implant bone remodeling, bone loss, esthetic outcomes, and, most importantly, patient satisfaction with the final restoration. No implant failures or prosthetic complications were reported, and all patients reported that they were very satisfied.5
Let’s look at two narrow-diameter implant case studies as examples.
Case Study No. 1
A 32-year-old male presented with a congenitally missing lateral, No. 10. The buccal-lingual dimensions were sufficient for standard implant placement, but the mesial-distal dimensions were 4.56 mm (figures 1a and 1b). The patient had a failing Maryland bridge, both functionally and esthetically (figure 2). He was always told that implants were not an option for him unless he underwent significant orthodontic treatment, and even then, nothing was guaranteed.
By selecting a 2.4 mm Anew implant (Dentatus), we were able to preserve sufficient bone between implant and tooth (1.5 mm), allowing for gingiva, a natural emergence profile, and maintaining the papilla in this highly esthetic area. Gingival recontouring was performed with a diode laser (Epic, Biolase). We had the lab fabricate a surgical guide and an immediate screw-retained provisional restoration for flapless implant placement (figures 3 and 4).
After a three-month integration period, final impressions were taken for a screw-retained crown. The procedure was noneventful, and not only was the patient happy having a provisional tooth, but the relief offered with a permanent fixed solution changed his entire outlook (figures 5 and 6).

Figure 1a: Pre-op panorex

Figure 1b: Pre-op CT scan

Figure 2: Failing Maryland bridge

Figure 3: Treatment software used to create surgical guide

Figure 4: Implant placement
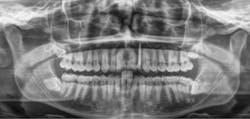
Figure 5: Post-op panorex

Figure 6: Final implant restoration
Case study No. 2
A 50-year-old female presented with a missing tooth No. 12 that was extracted for unknown reasons more than 10 years ago (figure 7). The patient was referred to our office for an implant consultation. Upon review of a CT scan, it was revealed that at the widest area buccal-lingually there was 4.09 mm and at the narrowest 3.8 mm (figure 8). She was presented with two treatment options: bone grafting or a narrow-diameter implant. She opted for the narrow-diameter implant, as it eased several of her concerns: she was unhappy with a removable appliance, worried about a block graft for a single tooth, and finances were a burden.

Figure 7: Pre-op panorex

Figure 8: Pre-op CT scan
A 1.8 mm x 14 mm Anew implant (Dentatus) was selected, and a surgical guide was fabricated for a flapless approach. In this instance, a healing cap was placed, and the existing flipper was relieved to address financial concerns (figures 9 and 10). A screw-retained crown was fabricated three months post insertion (figures 11 and 12). The patient reported no postoperative discomfort, and the case remains successful, as shown in the two-year postoperative x-ray (figure 13).

Figure 9: Implant placement

Figure 10: Implant exposed for impression

Figure 11: Final restoration

Figure 12: Final crown seating

Figure 13: Two-year follow-up
Further considerations
Narrow-diameter implants are an asset to any implant armamentarium. Patients should not be condemned to life with a removable appliance. These cases are just two small examples that highlight how we make the impossible a reality for patients who were previously denied implant treatment.
Many patients think that implants are too expensive. Because fewer procedures are required for narrow-diameter implants (e.g., no bone augmentation and fewer follow-up appointments), the cost is almost always significantly less expensive to the patient, while still preserving the fee for time and overhead for the practice.
Even when patients do have the financing in place, they are still cautious and looking for procedures that are significantly less time-consuming and forego surgical procedures. I use narrow-diameter implants that are conducive to one-stage, flapless surgery because they require one coring procedure. This allows us to maintain adequate bone volume and spacing for esthetic results. The unique screw-retained abutment reduces stress on the implant and provides for easy maintenance of provisional and long-term restorations. Perhaps the biggest bonus of all is being able to provide a greater number of patients with the same elevated, predictable level of care that was once denied them.
Narrow-diameter implants allow us to offer implant treatment to many more patients. It’s time to consider new ways of having an old discussion—let’s reframe the conversation about implants with patients who previously declined or were denied implant treatment.
References
1. The Oxford Dictionaries word of the year 2013. Oxford Dictionaries website. http://blog.oxforddictionaries.com/press-releases/oxford-dictionaries-word-of-the-year-2013/. Published November 19, 2013. Accessed September 1, 2017.
2. The top 50 European manufactures of dental implants (2nd ed.). Published by Research and Markets. 2013.
3. Dental implants facts and figures. American Academy of Implant Dentistry website. http://www.aaid.com/about/Press_Room/Dental_Implants_FAQ.html. Accessed May 31, 2017.
4. Christensen G, Child P. The truth about small diameter implants. Dentistry Today website. http://www.dentistrytoday.com/articles/178-articlesmagazine/dental-products/2646-the-truth-about-small-diameter-implants. Published May 1, 2010. Accessed September 1, 2017.
5. Froum SJ, Shi Y, Fisselier F, Cho SC, et al. Long-term retrospective evaluation of success of narrow-diameter implants in esthetic areas: A consecutive case series with 3 to 14 years follow-up. Int J Periodontics Restorative Dent. 2017;37(5):629-637.

Adam Koppelman, DMD, is a graduate of the University of Pennsylvania School of Dental Medicine. After completing a general practice residency at North Shore University Hospital, he continued working as chief resident and completed an implant and advanced prosthetics fellowship. He maintains a private practice in Manhattan, teaches at Columbia University, and serves as a volunteer on medical missions.