The future of dental practice — dental education
Eric Solomon, DDS, MA
The past 50 years have seen significant changes in the practice of dentistry. Evidence suggests we are going through a significant period of transition. The number of dental schools has increased, decreased, and then increased again, with related shifts in enrollment. These changes have propagated major shifts in the number and mix of dental care providers. Economic changes and changes in funding mechanisms for dental care have influenced the dental patient pool. Demographic and dental disease trends have prompted changes in the range of dental services provided and the characteristics of the dental patient population.
What will the dental practice of the future look like? The approach of this article will be to look at both historical data and projections in hope that they may provide insights into the dental practice of the future. Our glimpse into the future has four parts - dental enrollment trends, dental workforce trends, dental economic trends, and dental practice trends. This data should allow us to draw inferences as to the nature of dental practice in the future.
Dental education trends
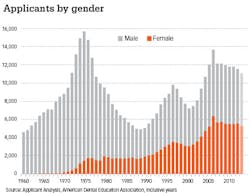
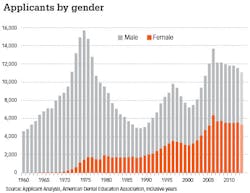
The number of applicants to dental school has impacted dental school enrollments significantly for the past half century. The applicant pool size can also serve as a surrogate measure of the general level of confidence in the future of the profession. Major shifts have occurred in the applicant pool over this time period (Figure 1). Between 1960 and 1975, the number of applicants to dental school more than tripled, increasing from 4,614 to 15,734 (11,070). This was followed by an almost identical decline of 10,738 applicants between 1975 and 1989. Several factors contributed to this decline, not the least of which was a soaring inflation rate during much of the period.
Since 1989, the applicant pool has only dropped below 8,000 twice, peaking at 13,722 in 2007. The number of applicants since 2007 had dropped slightly to 11,590 (-2,132) in 2013. However, preliminary data on the 2014 applicant pool indicate another drop this year. It is unlikely we will see a precipitous drop in applicants over the next few years. A career in dentistry has been rated highly compared to other career choices. This should help boost applicants' confidence in their choice of the dental profession.1 Female applicants have played a major role in the rise in the applicant pool. In 1960, there were only a handful of women who applied to dental school. In 2013, women represented almost half (48%) of all applicants.
The robust applicant pool has been a positive factor in encouraging higher education institutions to open their own dental schools. According to the American Dental Education Association, 14 dental schools have opened since 1997, raising the total number of schools to 66.2 In addition, there are at least 10 institutions of higher education that have formally expressed an interest in opening dental schools. It is highly unlikely that all these intentions will come to fruition; however, it is possible that some additional schools may open.
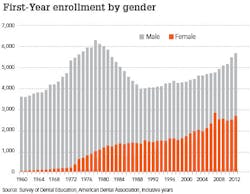
The trend in first-year enrollees mirrors the applicant trend to a large extent (Figure 2). Since 1960, first-year dental school enrollments have gone through three distinctly different periods (Figure 2). Between 1960 and 1978, first-year enrollment increased significantly from 3,616 to 6,301 (74%). During this time, 13 new dental schools were established, and encouraged by federal grants, existing schools increased their capacity. As in the applicant pool, the rapid rise in enrollment in the previous decade was matched with an equally dramatic decline between 1978 and 1989. By 1989, first-year enrollment had fallen to 3,979, a decrease of 2,322 students (-37%). To a large extent, the decline was fueled by a precipitous drop in the number of applicants to dental school and the withdrawal of federal support for enrollment expansion.
ADDITIONAL READING | Discover Dental School: Summer Scholars' Program
Largely as a consequence of the applicant decline, seven of the 60 dental schools had either closed or were in the process of closing by 1989. First-year enrollment has generally increased since 1989, rising to 5,697 in 2012 (1,718) with the largest increases in 2011 and 2012. Three new schools opened in 2011 and one in 2012. Given that three more schools opened in 2013 and that two more are slated to open in 2014, it is likely that first-year dental school enrollment will approach 6,000 by mid-decade. The growth in the number of female enrollees has been a significant trend. In 1960, females represented about 1% of the first-year class. By 2012, over 47% of the class was female.
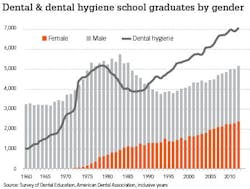
As you might expect, the pattern of dental school graduates generally follows that of first-year enrollment (Figure 3). From 1960 to 1976, the number of dental school graduates increased by 2,083 (64%). For the next decade, the number of graduates remained above 5,000. Between 1985 and 1993, graduates fell by 1,575 (-29%) to 3,778. Since 1993, graduates have increased to 5,199 (38%). Given the increases in first-year enrollment and the opening of new dental schools, the number of graduates is very likely to increase for the rest of the decade. Parallel to the trend in first-year enrollment, women now represent over 46% of the graduating class.
The trend in dental hygiene graduates mirrors the dental graduates up to 1986. At that point, dental school graduates continued to decline and hygiene graduates stabilized, then increased significantly. Between 1986 and 2012, hygiene graduates increased from 3,880 to 7,097, an increase of 3,217 (89%). It is difficult to predict how long this trend will continue. In 2012, there were 1.37 dental hygiene graduates for every dental graduate. The cost of educating a dental hygienist has decreased because of a change in the educational setting for the training of dental hygienists. In 1967, almost 40% of the dental hygiene programs were located in dental schools. In 2012, only 6.6% of the dental hygiene programs were located in dental schools, and only 12.2% of the programs awarded baccalaureate degrees.
ADDITIONAL READING | Tackling the Debt Monster: Why smarter choices in college equal easier days after graduation
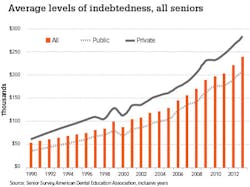
Dental student debt has soared since 1990 from an average of just over $50,000 to almost $250,000 in 2013 (Figure 4). These increases far exceed any inflationary trend during this period. Although higher, the rate of increase at private dental schools has been similar to the rate of increase at public dental schools. A major cause of this increase in indebtedness is shifting sources of dental school revenue. Driving this change is the dramatic decrease in the funding of dental schools by the states. In 1989, revenue from state sources accounted for 52.2% of total revenue for all dental schools. These funds shrunk to only 12.5% of revenue in 2012. The decrease in funding from the states is not unique to dental education but has affected all of higher education. Dental schools have been forced to raise revenue from other sources to compensate for this loss. For example, clinic revenue accounted for 15.6% of all revenue in 1989 and 20.1% of revenue in 2012. The largest increases, however, have been in dental school tuition, increasing from 23.7% of revenue in 1989 to 32.9% of revenue in 2012. The average tuition and fees for first-year dental students in 1989 was $8,867. By 2012, these costs had risen to $41,015. The increases in tuition have shifted the burden of funding dental education from the states to the students, and to a large extent, the increases account for the rise in student indebtedness.
The next article in this series will explore projections for the future of the dental workforce and examine how it has changed over the past half century.
References
1. Source: U.S. News & World Report, 1.23.14
2. http://www.adea.org/uploadedFiles/ADEA/Content_Conversion/publications/TrendsinDentalEducation2009/TDEEducational_Institutions/Documents/Educational_Institutions_Map_files/ADEAUSMemberInstitutions2014.pdf accessed 10/1/2014
Eric Solomon, DDS, MA, is a professor of Public Health Sciences at Texas A&M Health Science Center, Baylor College of Dentistry. He earned his bachelor's degree, master's degree, and dental degree from the University of Maryland. He also completed a general dentistry residency from the University of Rochester, a certificate in conflict resolution from The Texas A&M University System, and a graduate certificate in Geographic Information Systems from the University of Texas at Dallas. He has published over 130 articles in scholarly journals and has frequently been invited to speak on a wide variety of topics related to dental education and the future of dentistry.