INCREASING STAFF FUNCTIONS TO IMPROVE PRACTICE PRODUCTIVITY

Gordon J. Christensen, DDS, MSD, PhD
Q: In my state, a major third-party payment organization has recently reduced their payments by 15%. I am greatly concerned because my net revenue on most dental preventive and treatment procedures was already minimal, and my practice has not yet fully recovered from the recession. What can I do to increase revenue in this frustrating situation?
A: It is well known that the past few years have caused significant financial stress and frustration among dentists because of the reluctance of many patients to spend discretionary money for elective dental procedures. There are indications that the Great Recession is slowly coming to an end. However, with the exception of a few isolated geographic areas, it has been my observation when speaking in many national and international locations that the elective procedures dentists are doing have not yet returned to prerecession levels.
Third-party payment levels have been lowered in several states, reducing the remaining net income for dental practices. Additionally, midlevel dental practitioners have now been implemented in some areas, and they continue to be promoted by politicians and administrators, adding additional financial and clinical frustrations and challenges for some dentists. How can practicing dentists cope with these financial situations and the present and promoted changes in oral care delivery?
For several decades, I've been a strong proponent of expanding the clinical responsibilities of dental assistants and dental hygienists working under direct supervision of dentists. I feel that the well-proven, legally acceptable delegation of many clinical tasks to qualified staff persons is one of the most important ways for practicing dentists to cope with these challenges.
This column includes relatively new expanded functions, some controversial expanded functions, well-known staff functions still illegal in some locations, and long-recognized staff functions not delegated by some practitioners. Most of these staff functions have been incorporated into my practice for decades. Where legal, I suggest that they could be additionally implemented into the majority of general practices with the accompanying significant reduction in overhead costs and increased services to patients.
Potential expanded functions for dental hygienists and dental assistants
Many more expanded functions exist beyond the ones I will describe here. However, I've included those delegable tasks that allow dentists to accomplish clinical tasks that only they can do legally, while the staff person is the primary clinician for the delegated procedure.
After appropriate staff education and training, these tasks can become functions with which motivated staff persons can become extremely proficient. Most of the tasks are for either assistants or hygienists. Readers should check with their own local practice acts to ensure that the tasks are legal in their area. If they are not legal, I suggest that you initiate proposals to legalize them.
In my opinion, staff members who are directly supervised by dentists should accomplish these tasks as a part of an organized traditional dental team.
• Athletic mouthguards - (Fig. 1) This needed and neglected procedure becomes both a major service to patients and a significant source of staff-generated revenue. It can be promoted to patients, and parents with children who are athletes, and accomplished in-office by staff in a 30-minute appointment.

• Crown try-in - Some dentists are reluctant to have staff persons do this procedure. However, staff quickly becomes very proficient at observing marginal fit, contact area acceptability, anatomy, color, and occlusion of restorations. The 10-minute per seating savings of dentist time allows the dentist to come into the operatory after the staff person tries in the restoration, and seat the crown in a few minutes.
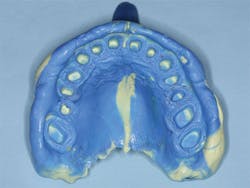
• Custom tray fabrication - (Figs. 2-3) Although it is estimated that only a minority of dentists use custom impression trays, actually many do so. Staff can easily and rapidly make these trays from light curing resin, thus saving significant laboratory expense, providing more accurate final impressions, and saving impression material because of the accurate fit of custom trays.

• Desensitization of teeth - There are numerous adequate desensitizing techniques for superficial tooth sensitivity. This task can be easily included into routine RDH responsibilities, since they are the ones who detect sensitivity during tooth scaling procedures.
• Diagnostic data collection - Collection of oral diagnostic data requires 30 to 60 minutes for patients who require even a moderate level of preventive and treatment procedures. I have delegated this procedure to staff with great success for several decades. The dentist is involved at the beginning of the appointment, and to develop the treatment plan after the staff person has completed the data collection.
• Educating patients - (Fig. 4) Effective use of staff to educate patients is the major key to practice success. Dentists should provide the necessary pamphlets, books, images, videos, and other educational information to staff, then conduct in-service education on the best ways to educate patients. Dentists simply reinforce and enhance the patient education.

• Fluoride application - This is an obvious staff responsibility, but it is my opinion that it is not promoted in many practices. Appropriate use of gels, varnishes, and systemic fluoride should be an everyday responsibility for staff persons.
• Laser therapy - Although both the adequacy of laser therapy in treatment of periodontal disease and the delegation of this task are controversial, this responsibility is legal for staff in some areas. Assuming the dentist and staff want to have laser therapy as part of their practice, and it is legal in their geographic area, it can be delegated to staff persons.
• Local anesthetic delivery - There are still a few states that do not allow this procedure. It is well proven and highly advantageous to delegate to qualified staff. Delegating this procedure allows dentists to use the time for other procedures that only they can legally accomplish.
• Occlusal splints - I estimate that about one-third of patients in a general practice have grinding or clenching bruxism. Making and delivering occlusal splints and making subsequent adjustments are a great service to patients and a significant staff revenue producer.
• Periodontal antibiotics - In some periodontal disease situations, so called "pocket stuffers" are used routinely. When indicated, this procedure has therapeutic value and can be easily delegated.
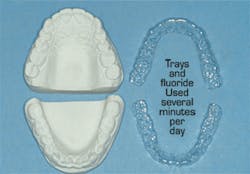
• Preventive appointment - (Fig. 5) I estimate that up to 10% of the patients in any general practice have one or more of the following conditions - senile caries, juvenile caries, bulimia, "meth mouth," chemotherapy, radiation therapy, and other conditions that require additional fluoride treatment provided in trays. This is an obvious staff educational and procedural task.
• Radiographs - Although almost all clinical staff persons make radiographs, I suggest that at least one person be designated as the one in charge of upkeep of the radiographic devices, and for keeping all staff members up to date about radiographic techniques. This person or persons can be responsible for making sure that all patients have adequate radiographs at the appropriate time intervals.
• Relining dentures temporarily - Relining complete or partial removable dentures for a temporary period is often necessary while implants are integrating or surgery sites are healing. Staff persons can easily accomplish this task, freeing dentists for other procedures.
• Restoration placement - Although legal in only a few states, this procedure, accomplished by educated and trained staff, has been shown over several decades to be a viable option. Again, I reinforce that it should be under direct supervision of a dentist. In most areas it is legal for provisional restorations to be made and cemented by staff members, saving the practitioner up to one half the crown preparation appointment time.
• Scaling and root planing - Dental hygienists are the major practitioners who provide this essential service. Due to the relatively low revenue produced for the time involved, delegation of this task is imperative to practice success, but some practices still do not do so. However, when expanding the roles of hygienists to include some of the other tasks described in this article, additional RDHs may be needed in the practice.
• Snore appliances - (Fig. 6) Sleep medicine is a growing concept in the profession, and I agree that it should be so. Qualified staff can be the major patient educators and providers of this service, assuming that proper sleep testing has been accomplished and staff have been educated.

• Sealant placement - This is an everyday procedure in almost every general practice. Education of parents about the value of sealants for their children and the availability of this procedure, as well as placement of the sealants, are all staff procedures.
• Whitening teeth in-office and supervision of at-home whitening - These are two of the most influential procedures to attract patients into additional esthetic dentistry procedures, and patient interest is high. The entirety of each procedure can and should be delegated to staff persons.
SUMMARY
I will summarize my suggestions to you. In recent years, dentists and many other health professionals have had to cope with significant, potentially negative financial situations caused by the recession and other commercial and governmental factors. The resultant reduction in patient activity and revenue production has negatively influenced the profession and the patients we serve. This article discussed significant ways that practitioners can reduce overhead and thus better cope with the financial challenges.
Delegation of many clinical tasks to qualified, educated, motivated staff persons working under the direct supervision of a dentist can significantly reduce the well-known current challenges.
Gordon Christensen, DDS, MSD, PhD, is a practicing prosthodontist in Provo, Utah. He is the founder and director of Practical Clinical Courses, an international continuing-education organization initiated in 1981 for dental professionals. Dr. Christensen is a cofounder (with his wife, Dr. Rella Christensen) and CEO of CLINICIANS REPORT (formerly Clinical Research Associates).
In this monthly feature, Dr. Gordon Christensen addresses the most frequently asked questions from Dental Economics readers. If you would like to submit a question to Dr. Christensen, please send an email to [email protected].