Increasing the longevity of Class II resin-based composites

By Gordon J. Christensen, DDS, MSD, PhD
Q After placing Class II resin-based composites for many years, I'm convinced that the longevity of these restorations is relatively short. What am I doing wrong? Can the longevity of these restorations be increased?
A I have placed Class II composites since their inception in the profession, and I have personally observed the less than desirable longevity of these restorations when compared to metal restorations or crowns. I have identified numerous clinical factors in the Class II composite technique that could be modified to improve their longevity. However, I also see some negative factors that are almost impossible for practitioners to control. I'll discuss these characteristics.
In my opinion, the international research on the subject is so varied and confounded that it is more confusing than useful when compared to the knowledge of an experienced long-time practitioner. For example, some studies include restorations representing the clinical activity of only one practitioner, obviously showing only the expected clinical results for that specific practitioner. Other studies are retrospective and observe the clinical results of a group of private practitioners in a specific geographic area, while others are highly controlled in academic environments without the financial and other well-known challenges, restraints, and impediments of real-world practice. If you were to peruse the references available in the literature, you would be enlightened about composite longevity, but only to the diversity of the results and the lack of unanimous conclusions on most of the aspects of this topic.
My answer includes my personal observations, the clinical conclusions of dentists in study clubs for which I'm a mentor, and research information in the literature. Some of the literature agrees with the clinical observations of experienced clinicians concerning improving the longevity of Class II resin-based composite restorations, while some contradicts it. Included is research information from the literature instructing dentists based on in-vitro research or varied clinical studies. However some of the studies are not in agreement with what some call "practice-based evidence." I strongly believe that both scientific studies and clinical observation are necessary to make clinical decisions. My answer reflects that belief.
Inability to easily identify initial interproximal carious lesions
Large Class II composite restorations fail more often and faster than small ones. However, it is difficult to detect small interproximal carious lesions. Current digital sensors DO NOT show initial lesions well. The manufacturers of digital sensors need to develop sensors that show the actual depth of incipient carious lesions without having to purchase additional software. Any observant clinician knows that the current sensors used as meticulously as possible show only about half of initial interproximal lesions, even when enlarging the image, or using colorization or texturing. Some additional software such as Logicon (from Carestream Dental, Atlanta) helps interpret small lesions by evaluating the differences between the various shades of gray in the image, but only a few dentists have such software. Several other digital interproximal caries detection devices are available or are under development, but the available ones are expensive and not used by many dentists. The result is that lesions often go unnoticed until they are large. I've seen many interproximal lesions up to 2 mm and 3 mm deep that are barely perceptible on digital radiographs. Large Class II composites do not serve as long or as well as small ones. (Fig. 1) Dentists and manufacturers should diligently look for more adequate sensors and other methods to allow detection of incipient carious lesions.

Large burs cut away too much tooth structure
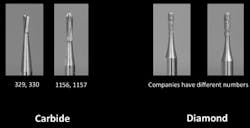
Many years ago, before the advent of the air rotor, large crosshatched carbide burs with right angles on the cutting end, such as Nos. 557 and 558, were popular. Some dentists still use them, often making every Class II preparation larger than necessary. Survey and in-vitro research shows that small, round-ended burs such as Nos. 329, 330, and 245 are the most popular. (Fig. 2) In the U.S., carbide burs are used far more than diamond burs for Class II tooth preparations, but in many countries diamond burs are most popular. There appears to be little difference in the clinical result whether using diamond or carbide burs. The logical conclusion relative to burs is that small burs should be used for preparation of incipient lesions, but this conclusion brings another challenge -- nicking adjacent teeth. It has been shown that adjacent teeth are nicked by most dentists when cutting Class II preparations. This problem can be avoided by placing a simple metal shield between the teeth, such as a WedgeGuard (Triodent, KatiKati, New Zealand), or FenderWedge (Garrison, Spring Lake, MI) to prevent the nicks.
Making large tooth preparations for incipient carious lesions can be avoided by using small burs, but nicking adjacent teeth with any type of bur is preventable by using metal guards as described above to protect the adjacent tooth. We dentists can do a better job when accomplishing Class II composite restorations by detecting carious lesions when they are small, and by using small instruments when removing the carious tooth structure.
What are the advantages of small tooth preparations for patients and dentists?
The patient advantages of small tooth preparations
Many patients do not visit their dentists on a regular basis, and their carious lesions are already too large when they finally get to the dentist. For these patients, there is no alternative to making large restorations. I strongly suggest tactfully informing them that their large restorations will have shorter longevity than they would have if they had been detected sooner. This could help motivate them to visit their dentists more frequently.
However, in a practice where patients are examined every few months, small lesions can usually be detected early in their development. When the lesions are small, the tooth preparations can be similarly small.
Advantages of small Class II tooth preparations for the patient are clear -- the restorations serve longer as described above. Additionally, the smaller the isthmus cut, the stronger the remaining tooth structure as discussed. The expectation is that the stronger tooth structure remaining will also last longer without breaking during chewing. Every clinical dentist sees restored teeth with fractured cusps on a routine basis.
When treating incipient lesions, dentists are advised to take a photo of the lesion as it is entered with the bur. Such photos may be requested by third-party payment companies to justify making the small tooth preparation and restoring the incipient lesion.
The dentist advantages of small tooth preparations
Although there are many differences in the operating speed of dentists, typical experienced dentists require about 15 to 20 minutes for a small Class II composite restoration, while larger composite restorations can require up to twice as much time. (Fig. 3) Third-party payment companies do not have different designations or fees for small or large MOD restorations. A large Class II restoration receives the same remuneration to the dentist as a small restoration.
Most dentists agree that it is more difficult to prepare and restore a large tooth preparation with composite than it is to prepare and restore a small tooth preparation. They also agree that large composite restorations are among the most difficult procedures to accomplish, since they must restore tight contact areas, and achieve adequate occlusion, closed margins, and sealed dentin to prevent postoperative tooth sensitivity. All of these tasks must be done quickly because of the low revenue generated by this procedure and the high overhead of dental practices. Placing these restorations all day long is a genuinely fatiguing and often unrewarding task. I suggest integrating them with some less stressful clinical procedures. Small tooth preparations allow faster and easier procedures for the restorative dentist.

Another advantage of small tooth preparations for dentists is that the material cost for small restorations is significantly less than for large restorations. Since the revenue generated for typical Class II composite restorations is relatively small when compared to the fees for some other procedures, the reduction in material cost helps reduce the overhead cost when placing Class II restorations.
Summary
Class II resin-based composite restorations do not have impressive longevity as based on clinical observation of experienced restorative dentists and the general conclusion of the scientific literature on this subject. The larger the Class II composite, the less time it's expected to serve. Current digital radiographic sensors do not demonstrate initial carious lesions as adequately as desired, thereby forcing dentists to make tooth preparations larger than necessary. Some dentists are cutting tooth preparations that are larger than necessary because they use large burs. Small burs are suggested. Many patients force dentists to make large tooth preparations because they do not visit their dentists frequently and the carious lesions become larger than desirable before detection. The answer to the title of this article is YES!
Class II resin-based composite restorations can have longer service potential using the concepts discussed!
Gordon Christensen, DDS, MSD, PhD, is a practicing prosthodontist in Provo, Utah. He is the founder and director of Practical Clinical Courses, an international continuing-education organization initiated in 1981 for dental professionals. Dr. Christensen is a cofounder (with his wife, Dr. Rella Christensen) and CEO of CLINICIANS REPORT (formerly Clinical Research Associates).
In this monthly feature, Dr. Gordon Christensen addresses the most frequently asked questions from Dental Economics® readers. If you would like to submit a question to Dr. Christensen, please send an email to [email protected].
ADDITIONAL RESOURCES
PRACTICAL CLINICAL COURSES has many professional videos on almost all dental subjects. Our recent video, V3554, Class II Composite Resins Can Be Predictable, Non-Sensitive, and Profitable, shows Dr. Christensen placing composites using the best products in each category of the technique. The close-up, live, one-hour video demonstration makes placing composites relatively simple and predictable.
A companion video, V1559 Direct Resin Veneers, shows the easiest and most adequate way and the best materials to place economical composite veneers in this frustrating economic time.
In our two-day hands-on course, Successful Real-World Practice -- Restorative Dentistry, you actually place these restorations as well as practice several other procedures, including resin veneers.
For information, call (800) 223-6569 or go to www.pccdental.com.
Past DE Issues