Treating patients who have minimal ability to pay

By Gordon J. Christensen, DDS, MSD, PhD
Q Although the great recession is supposed to be over, it's still clearly present in my town. I have many patients who before the recession could afford to pay for crowns or other expensive dentistry, but they are now unable to do so. What can be done for these people, since we hope they will eventually be able to afford dental treatment again, and we do not want to extract their teeth?
A The situation you described is always present, whether there's a recession or not. Some patients cannot afford dental care, but they want to retain their teeth. I've always had many patients with financial challenges, as do most dentists. There are ways to help these patients. They are usually very grateful at the time of treatment, and many in my practice have become long-time, normal patients as they have become more financially stable.
I will provide my opinions for you, and I suggest that you consider them and change them to fit your own patients and geographic location.

The first and probably most important step is to take care of the emergency treatment as soon as possible, removing obviously destroyed teeth, placing temporary restorations in salvageable teeth, and accomplishing whatever emergency periodontal treatment is necessary. If this preliminary treatment necessitates removal of teeth in esthetically sensitive locations, inexpensive removable partial dentures (flippers) should be placed to allow a patient to appear as normal as possible. At this point in the treatment, the patient's oral condition should not have any emergency needs, the person should not be in a painful state, and you should have provided the treatment as inexpensively as possible.

The second step, just as important as the first step, is to get the patient started on a preventive program that will maintain the treatment as long as possible. The new preventive orientation will allow the person to recover from the financial challenge of the emergency treatment, and to save funds for future and longer-lasting treatment. What preventive treatment is desirable for such patients?

Most of these patients have not developed oral hygiene or dietary habits that are conducive to low dental caries rates. However, all of us know that changing the behavior of an adult is almost impossible. Preventive measures that do not require major behavior changes are the most successful. What does that mean?

Most people brush their teeth at least once a day using the most popular and readily available toothpastes that contain about 1,000 ppm fluoride ions. These toothpastes are only moderately effective in reducing dental caries. Get patients to use more effective preventive toothpastes containing 5,000 ppm fluoride, which are proven to further reduce or even eliminate additional dental caries. Examples are PreviDent 5000 from Colgate, and ClinPro 5000 from 3M ESPE. These stronger toothpastes are a bit expensive, and in most countries require a prescription. I suggest that you buy the toothpastes in quantity and provide them to your high caries patients at your cost or a slight profit. Now, you have NOT changed their tooth brushing behavior, but you have provided more effective caries control for them at slightly more cost. Suggest that their most important brushing time should be just before bedtime to allow the toothpaste residue to rest on their teeth during the night.

Of course, flossing should also be encouraged and demonstrated to patients. However, it's doubtful that flossing will be accepted by patients who were not flossing before.

I suggest that you also make some simple dietary recommendations that have been well proven over the past several decades. These should not require major behavior changes or patients will not follow them. Examples are:
- Reduce sticky, sugary foods.
- When eating sticky, sugary foods, eat them all at once, preferably at mealtime, rather than eating them over a prolonged period of time. Frequent eating of these high caries-promoting foods allows them to remain on the teeth longer and does not let the mouth recover from the sugar saturation.
- If possible, clean the sticky food debris from the mouth immediately after eating it.
- When eating sugar-rich foods, do so at meals instead of between meals to reduce sugar saturation on the teeth.
- Reduce high sugary sodas or fruit juices.
- When drinking high sugary sodas or fruit juices, drink them all at once rather than sipping them over a period of time.
- Use high fluoride toothpastes.
- Never skip brushing the teeth just before bedtime or any other times during the day that you normally brush. Debris that has been on teeth more than 24 hours has been proven to be destructive.
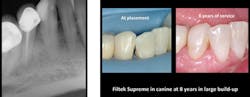
At this point in the treatment, patients should be able to begin a slow and relatively inexpensive way to restore the teeth that had provisional restorations placed in them. Although the carious lesions are large and would be better restored with crowns, consider the following procedure due to the patient's financial limitations. Use build-up techniques on the affected teeth with conventional esthetic restorative materials instead of the relatively unesthetic typical build-up resin-based composites. Most patients have dental benefit plans. Bill these restorations as build-ups (code 2950), not as final restorations. When a patient has adequate financial ability, crowns should be done.

The following images show a patient with limited finances but a strong desire to retain her teeth. The crowns present in the quadrant placed by a previous dentist show that the patient at one time had adequate finances for crowns.
The technique for building up restorations to restore deep carious lesions follows:
You and I recognize that in this strained financial time many patients do not have the financial resources to proceed with expensive options. Recently we made a video showing how patients with limited financial resources could afford to have oral rehabilitation spread out over several years. I have done this hundreds of times to allow such people to have the benefits of modern dentistry in spite of their financial limitations.
To summarize my answer, there are well proven ways to treat patients with limited financial resources. I have provided my suggestions concerning how to accommodate such patients and still retain many of their teeth.
I strongly feel that there are more patients in this category than in the financially affluent category, and that it is our professional responsibility to offer affordable plans for them.
I wish you success in initiating this concept into your practice.
Gordon Christensen, DDS, MSD, PhD, is a practicing prosthodontist in Provo, Utah. He is the founder and director of Practical Clinical Courses, an international continuing-education organization initiated in 1981 for dental professionals. Dr. Christensen is a cofounder (with his wife, Dr. Rella Christensen) and CEO of CLINICIANS REPORT (formerly Clinical Research Associates).
In this monthly feature, Dr. Gordon Christensen addresses the most frequently asked questions from Dental Economics® readers. If you would like to submit a question to Dr. Christensen, please send an email to [email protected].
Recently we made a video showing segmented treatment for a patient with minimal financial resources and the desire to maintain remaining teeth. The video is "Affordable Treatment of Complex Rehabilitative Needs." Item V1964.
This one-hour video shows how to allow your financially stressed patients afford excellent oral rehabilitative treatment using segmented treatment plans.
Go to www.pccdental.com or call (800) 223-6569 for additional information.
Past DE Issues