Which indirect restorations do dentists want in their own mouths?
by Gordon J. Christensen, DDS, MSD, PhD
Q It is apparent that the major emphasis for indirect restorations promoted by laboratories and manufacturers is toward ceramic crowns for all locations in the mouth. Maybe I am behind the trend, but that does not seem logical to me. What is the current use of materials for indirect crowns and fixed prostheses? Has porcelain-fused-to-metal been replaced? Is it still acceptable to use cast gold alloy restorations?
A I hear this question frequently. My answer will not be simple. Yes, the trend is definitely toward using full-ceramic indirect restorations for everything. Whether or not it is a correct trend is still to be determined by long-term clinical research and practitioner observation. Numerous reasons have influenced this very obvious movement to full-ceramic restorations.
The public we serve wants and demands tooth-colored restorations
That statement is not even debatable. In the past, many patients requiring crowns were satisfied to have long-lasting cast gold alloy inlays, onlays, partial crowns, full crowns, and fixed prostheses. These restorations served for several decades, but with a few exceptions, only dentists considered them to be acceptable from an esthetic standpoint.
Currently, very few patients will accept gold alloy restorations in spite of their proven longevity. It has been revealing to note that, with few exceptions, patients prefer tooth-colored indirect restorations even after being told that they usually have shorter service longevity than gold alloy restorations. I do not see this changing. In fact, I predict that it will become more prevalent.
The cost of gold alloy and other alloys is extremely high and unstable
There is no question that gold, platinum, palladium, and other elements have increased in cost to the level that their use as tooth restorations is questionable. Large crowns that have gold alloy content often increase crown cost 20% or more than a full-ceramic alternative.
The cost of full-ceramic crowns from laboratories is at an all-time low
Offshore dental laboratories and some American laboratories have reduced the cost of zirconia, zirconia-based, and lithium disilicate restorations to unprecedented levels. The current low laboratory cost for full-ceramic crowns is another significant reason why gold alloy crowns are used less. The cost of typical full-ceramic crowns has now reduced about 30% or 40% below average crown costs before the great recession. These lower costs compensate somewhat for the increased taxes placed on dental laboratory products by the federal government. However, passing on any further reduction in laboratory costs to patients is a logical suggestion. Dentists are opting for lower cost full-ceramic crowns.
Some of the new full-ceramic restorations are easy to fabricate
Milling indirect restorations has become commonplace. The majority of American dental laboratories are now able to mill restorations, and it will be only a short time until all dental laboratories will be capable of milling restorations. This concept greatly reduces the human involvement that was previously necessary for fabricating indirect restorations, and therefore, reduces the cost.
Are the current ceramic indirect restorations well proven clinically?
Since they have only been used clinically for a few years, it is too early to have long-term clinical research on some of the new ceramic formulations.
- IPS e.max and zirconia-based restorations have had a decade or more of clinical observation in some investigations.
- Full-zirconia restorations have had only a few years of clinical observation, and in spite of most dentists using them routinely, they still need several more years of observation for both single units and connected multiple units.
- New forms of tooth-colored restorations, such as a resin-nano ceramic (Lava Ultimate from 3M ESPE) or a hybrid ceramic (ENAMIC from VITA), are now classified as "ceramics"for third-party payment and look very promising. However, they also require significant additional long-term clinical research.
How long is long enough to watch these new restorations clinically? That is a controversial question. Cast gold restorations have been observed for many decades, and most dentists conclude that when fabricated and cemented properly, cast gold will serve almost indefinitely. Porcelain-fused-to-metal (PFM) restorations have been observed for 50 years, and clinical conclusions can be made about the potential longevity of crowns and fixed prostheses. In my opinion, we need at least 10 years of controlled observation for enough evidence to feel comfortable with almost any new treatment, including indirect restorations. When considering the available research literature, it can easily be concluded that more research is needed on the current generation of full-ceramic crowns.
I suggest that practitioners limit the use of the newer restorations to only some of their treatment. They should observe them carefully, while continuing to use the previous indirect restorations with which they’ve had clinical success. Each dentist can draw his or her own conclusions about the viability of the new types of restorations as new controlled research comes forth.
Complete patient education and informed consent about the new restorations should be obtained from patients before proceeding. They should know these restorations have been used only for a short time.
What are the best restorations for specific sites in the mouth?
This question is a controversial one. It depends on esthetic demands of the patient, severity of occlusion, cost of restorations from laboratories, age of the patient, oral hygiene history, caries susceptibility, and patient preferences. On polling dentists in continuing education courses about the restorations they would prefer in their own mouths, the following preferences were expressed to me (listed in decreasing order of preference for each type of tooth):
- Second molars, maxillary and mandibular – cast gold, nearly unanimous
- First molars mandibular – cast gold, PFM, full-zirconia
- First molars maxillary – IPS e.max, PFM, full-zirconia
- Premolars, maxillary and mandibular – IPS e.max, PFM, full-zirconia
- All six anterior maxillary or mandibular teeth at one time – IPS e.max
- One anterior tooth with other acceptable natural teeth present – IPS Empress
Which new crown type is most popular?
Use of full-zirconia restorations is growing rapidly, faster than other new tooth-colored restorations. The new technology and research that is being introduced into zirconia restorations will soon allow zirconia to have near optimum esthetics. Any tooth color desired accompanied with optimum esthetics will soon be available. I predict that the growth of zirconia will continue to outpace the growth of other new tooth-colored restorations.
Summary
It is clear to any observer that cast gold alloy and PFM restorations have reduced significantly in use. Full-zirconia, IPS e.max, and zirconia-based restorations are now the most popular indirect restorations in many practices. My suggestion is to use the new restorations with caution, not totally replacing PFM or cast gold alloy. When these restorations have whatever number of years you consider appropriate for clinical evidence, that will be the time to shift completely.
Gordon Christensen, DDS, MSD, PhD, is a practicing prosthodontist in Provo, Utah. He is the founder and director of Practical Clinical Courses, an international continuing-education organization initiated in 1981 for dental professionals. Dr. Christensen is a cofounder (with his wife, Dr. Rella Christensen) and CEO of CLINICIANS REPORT (formerly Clinical Research Associates).
In this monthly feature, Dr. Gordon Christensen addresses the most frequently asked questions from Dental Economics® readers. If you would like to submit a question to Dr. Christensen, please send an email to [email protected].
Practical Clinical Courses (PCC)
has numerous educational programs to help you understand this subject better. I suggest the following:
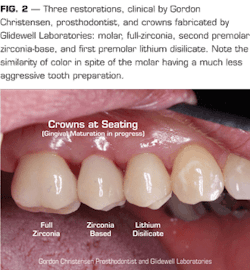
A one-hour video, "Zirconia and Lithium Disilicate restorations – Clinical Comparison and Techniques"(Item V1956)
A two-day hands-on course in Utah, "Successful Real-World Practice-Fixed Prosthodontics"www.pccdental.com or by calling (800) 223-6569.
Past DE Issues